

Evidence on Technology-Based Psychological Interventions in Diagnosed Depression: Systematic Review
- PMID: 33565981
- PMCID: PMC7904404
- DOI: 10.2196/21700
Evidence on Technology-Based Psychological Interventions in Diagnosed Depression: Systematic Review
Abstract
Background: Evidence on technology-based psychological interventions (TBIs) for the treatment of depression is rapidly growing and covers a broad scope of research. Despite extensive research in this field, guideline recommendations are still limited to the general effectiveness of TBIs.
Objective: This study aims to structure evidence on TBIs by considering different application areas (eg, TBIs for acute treatment and their implementation in health care, such as stand-alone interventions) and treatment characteristics (eg, therapeutic rationale of TBIs) to provide a comprehensive evidence base and to identify research gaps in TBIs for diagnosed depression. Moreover, the reporting of negative events in the included studies is investigated in this review to enable subsequent safety assessment of the TBIs.
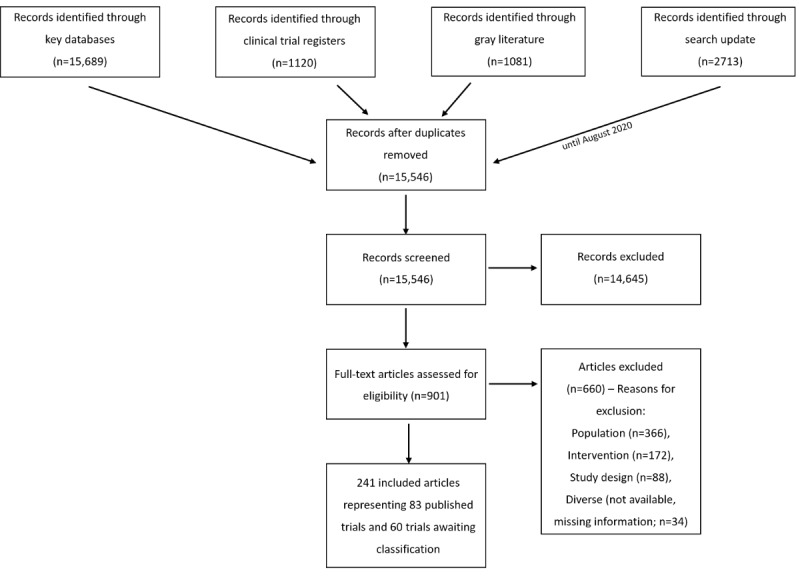
Methods: Randomized controlled trials on adults diagnosed with unipolar depression receiving any kind of psychotherapeutic treatment, which was at least partly delivered by a technical medium, were eligible for inclusion in our preregistered systematic review. We searched for trials in CENTRAL (Cochrane Central Register of Controlled Trials; until August 2020), MEDLINE, PsycINFO, PSYNDEX, CINAHL; until the end of January 2018), clinical trial registers, and sources of gray literature (until the end of January 2019). Study selection and data extraction were conducted by 2 review authors independently.
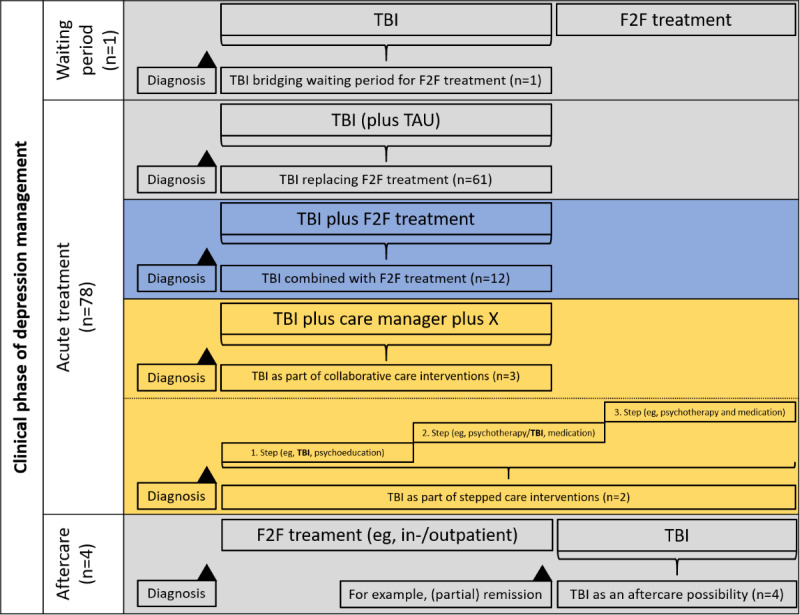
Results: Database searches resulted in 15,546 records, of which 241 publications were included, representing 83 completed studies and 60 studies awaiting classification (ie, preregistered studies, study protocols). Almost all completed studies (78/83, 94%) addressed the acute treatment phase, being largely either implemented as stand-alone interventions (66/83, 80%) or blended treatment approaches (12/83, 14%). Studies on TBIs for aftercare (4/83, 5%) and for bridging waiting periods (1/83, 1%) were scarce. Most TBI study arms (n=107) were guided (59/107, 55.1%), delivered via the internet (80/107, 74.8%), and based on cognitive behavioral treatment approaches (88/107, 79.4%). Almost all studies (77/83, 93%) reported information on negative events, considering dropouts from treatment as a negative event. However, reports on negative events were heterogeneous and largely unsystematic.
Conclusions: Research has given little attention to studies evaluating TBIs for aftercare and for bridging waiting periods in people with depression, even though TBIs are seen as highly promising in these application areas; thus, high quality studies are urgently needed. In addition, the variety of therapeutic rationales on TBIs has barely been represented by identified studies hindering the consideration of patient preferences when planning treatment. Finally, future studies should use specific guidelines to systematically assess and report negative events.
Trial registration: International Prospective Register of Systematic Reviews (PROSPERO) CRD42016050413; https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42016050413.
International registered report identifier (irrid): RR2-10.1136/bmjopen-2018-028042.
Keywords: depression; depressive disorder; internet; mobile phone; psychotherapy; systematic review; telephone.
©Moritz Köhnen, Mareike Dreier, Tharanya Seeralan, Levente Kriston, Martin Härter, Harald Baumeister, Sarah Liebherz. Originally published in JMIR Mental Health (http://mental.jmir.org), 10.02.2021.
Conflict of interest statement
Conflicts of Interest: HB received consultancy fees, reimbursement of congress attendance, and travel costs as well as payments for lectures from psychotherapy and psychiatry associations as well as psychotherapy training institutes in the context of e–mental health topics. He has been the beneficiary of study support (third-party funding) from several public funding organizations. HB and MH participated in the current revision of the German S3 national clinical practice guideline on the treatment of adults with unipolar depression. MH and LK participated in the 2015 revision of the German S3 national clinical practice guideline on the treatment of adults with unipolar depression. MH and SL are licensed psychotherapists. SL is additionally employed at the institute for psychotherapy at the University Medical Center Hamburg-Eppendorf, which provides psychotherapist training in CBT. MK and MD are psychotherapists in training (CBT). TS is a psychotherapist in training (psychodynamic therapy).
Figures
References
-
- DGPPN. BÄK. KBV. AWMF for the guideline group unipolar depression S3 Guideline/National Disease Management Guideline Unipolar Depression – Long Version, 2nd edition. Version 5. 2015. www.depression.versorgungsleitlinien.de.
-
- Kessler RC, Nelson CB, McGonagle KA, Liu J, Swartz M, Blazer DG. Comorbidity of DSM-III-R major depressive disorder in the general population: results from the US National Comorbidity Survey. Br J Psychiatry Suppl. 1996 Jun;168(30):17–30. - PubMed
-
- Hare DL, Toukhsati SR, Johansson P, Jaarsma T. Depression and cardiovascular disease: a clinical review. Eur Heart J. 2014 Jun 1;35(21):1365–72. doi: 10.1093/eurheartj/eht462. http://eurheartj.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=24282187 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
