

Pacemaker lead-associated tricuspid regurgitation in patients with or without pre-existing right ventricular dilatation
- PMID: 33566185
- PMCID: PMC8166708
- DOI: 10.1007/s00392-021-01812-3
Pacemaker lead-associated tricuspid regurgitation in patients with or without pre-existing right ventricular dilatation
Abstract
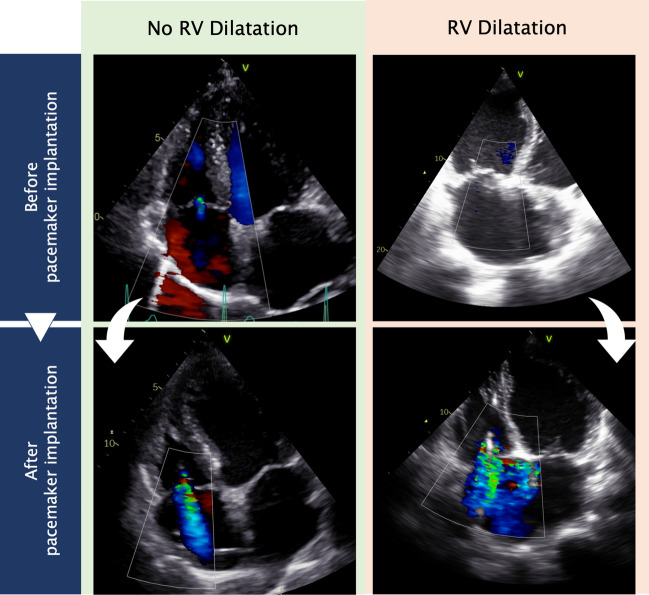
Background: Transcatheter tricuspid valve intervention became an option for pacemaker lead-associated tricuspid regurgitation. This study investigated the progression of tricuspid regurgitation (TR) in patients with or without pre-existing right ventricular dilatation (RVD) undergoing pacemaker implantation.
Methods: Patients were included if they had implantation of transtricuspid pacemaker lead and completed echocardiography before and after implantation. The cohort was divided in patients with and without RVD (cut-off basal RV diameter ≥ 42 mm). TR was graded in none/mild, moderate, and severe. Worsening of one grade was defined as progression. Survival analyses were plotted for 10 years.
Results: In total, 990 patients were analyzed (24.5% with RVD). Progression of TR occurred in 46.1% of patients with RVD and in 25.6% of patients without RVD (P < 0.001). Predictors for TR progression were RV dilatation (OR 2.04; 95% CI 1.27-3.29; P = 0.003), pre-existing TR (OR 4.30; 95% CI 2.51-7.38; P < 0.001), female sex (OR 1.68; 95% CI 1.16-2.43; P = 0.006), single RV lead (OR 1.67; 95% CI 1.09-2.56; P = 0.018), mitral regurgitation (OR 2.08; 95% CI 1.42-3.05; P < 0.001), and enlarged left atrium (OR 1.98; 95% CI 1.07-3.67; P = 0.03). Survival-predictors were pacemaker lead-associated TR (HR 1.38; 95% CI 1.04-1.84; P = 0.028), mitral regurgitation (HR 1.34; 95% CI 1.02-1.77; P = 0.034), heart failure (HR 1.75; 95% CI 1.31-2.33; P < 0.001), kidney disease (HR 1.62; 95% CI 1.25-2.11; P < 0.001), and age ≥ 80 years (HR 2.84; 95% CI 2.17-3.71; P < 0.001).
Conclusions: Patients with RVD receiving pacemaker suffered from increased TR progression, leading to decreased survival.
Keywords: Device complications; Pacemaker; Right ventricle; Tricuspid regurgitation; Valvular heart disease.
Conflict of interest statement
Martin Andreas has served as a Proctor for Edwards and Abbott, served as an Advisor for Medtronic and reported receiving Institutional Grants from LSI, Abbott, Edwards, and Medtronic during the conduct of the study. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures


References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
