

Total Thyroidectomy Versus Lobectomy for Thyroid Cancer: Single-Center Data and Literature Review
- PMID: 33566240
- PMCID: PMC8253713
- DOI: 10.1245/s10434-020-09481-8
Total Thyroidectomy Versus Lobectomy for Thyroid Cancer: Single-Center Data and Literature Review
Abstract
Background: Controversies remain about the ideal risk-based surgical approach for differentiated thyroid cancer (DTC).
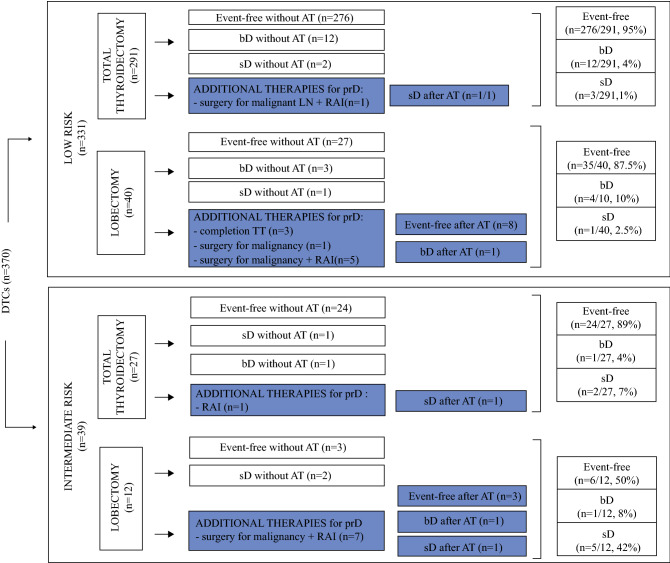
Methods: At a single tertiary care institution, 370 consecutive patients with low- or intermediate-risk DTC were submitted to either lobectomy (LT) or total thyroidectomy (TT) and were followed up.
Results: Event-free survival by Kaplan-Meier curves was significantly higher after TT than after LT for the patients with either low-risk (P = 0.004) or intermediate-risk (P = 0.032) tumors. At the last follow-up visit, the prevalence of event-free patients was higher in the TT group than in the LT low-risk group (95% and 87.5%, respectively; P = 0.067) or intermediate-risk group (89% and 50%; P = 0.008). No differences in persistence prevalence were found among microcarcinomas treated by LT or TT (low risk, P = 0.938 vs. intermediate-risk, P = 0.553). Nevertheless, 15% of the low-risk and 50% of the intermediate-risk microcarcinomas treated by LT were submitted to additional treatments. On the other hand, macrocarcinomas were significantly more persistent if treated with LT than with TT (low-risk, P = 0.036 vs. intermediate-risk, P = 0.004). Permanent hypoparathyroidism was more frequent after TT (P = 0.01). After LT, thyroglobulin (Tg)/thyroid-stimulating hormone (TSH) had shown decreasing trend in 68% of the event-free patients and an increasing trend in the persistent cases.
Conclusions: Lobectomy can be proposed for low-risk microcarcinomas, although in a minority of cases, additional treatments are needed, and a longer follow-up period usually is required to confirm an event-free outcome compared with that for patients treated with TT. On the other hand, to achieve an excellent response, TT should be favored for intermediate-risk micro- and macro-DTCs despite the higher frequency of postsurgical complications.
Conflict of interest statement
There are no conflicts of interest.
Figures


Similar articles
-
Dynamic Risk Stratification in Patients with Differentiated Thyroid Cancer Treated Without Radioactive Iodine.J Clin Endocrinol Metab. 2016 Jul;101(7):2692-700. doi: 10.1210/jc.2015-4290. Epub 2016 Mar 29. J Clin Endocrinol Metab. 2016. PMID: 27023446 Free PMC article.
-
Surgical Management of Low-/Intermediate-Risk Node Negative Thyroid Cancer: A Single-Institution Study Using Propensity Matching Analysis to Compare Thyroid Lobectomy and Total Thyroidectomy.Thyroid. 2022 Jan;32(1):28-36. doi: 10.1089/thy.2021.0356. Thyroid. 2022. PMID: 34861772 Free PMC article.
-
Total thyroidectomy versus lobectomy for intermediate-risk papillary thyroid carcinoma: A single-institution matched-pair analysis.Oral Oncol. 2019 Mar;90:17-22. doi: 10.1016/j.oraloncology.2019.01.010. Epub 2019 Jan 31. Oral Oncol. 2019. PMID: 30846171
-
Continuing controversy regarding individualized surgical decision-making for patients with 1-4 cm low-risk differentiated thyroid carcinoma: A systematic review.Eur J Surg Oncol. 2020 Dec;46(12):2174-2184. doi: 10.1016/j.ejso.2020.08.014. Epub 2020 Aug 28. Eur J Surg Oncol. 2020. PMID: 32933805
-
Is thyroglobulin a reliable biomarker of differentiated thyroid cancer in patients treated by lobectomy? A systematic review and meta-analysis.Clin Chem Lab Med. 2022 Apr 28;60(7):1091-1100. doi: 10.1515/cclm-2022-0154. Print 2022 Jun 27. Clin Chem Lab Med. 2022. PMID: 35475431
Cited by
-
Poorly Differentiated Thyroid Carcinoma in a 19-Year-Old Young Female Patient: A Case Report.Cureus. 2024 Jul 22;16(7):e65149. doi: 10.7759/cureus.65149. eCollection 2024 Jul. Cureus. 2024. PMID: 39176351 Free PMC article.
-
Risk Factors for Calcium-Phosphate Disorders after Thyroid Surgery.Biomedicines. 2023 Aug 18;11(8):2299. doi: 10.3390/biomedicines11082299. Biomedicines. 2023. PMID: 37626794 Free PMC article.
-
Current practice in intermediate risk differentiated thyroid cancer - a review.Rev Endocr Metab Disord. 2024 Feb;25(1):95-108. doi: 10.1007/s11154-023-09852-y. Epub 2023 Nov 23. Rev Endocr Metab Disord. 2024. PMID: 37995023 Review.
-
Initial versus Staged Thyroidectomy for Differentiated Thyroid Cancer: A Retrospective Multi-Dimensional Cohort Analysis of Effectiveness and Safety.Cancers (Basel). 2024 Jun 18;16(12):2250. doi: 10.3390/cancers16122250. Cancers (Basel). 2024. PMID: 38927955 Free PMC article.
-
Association between surgical extent and recurrence in unilateral intermediate- to high-risk papillary thyroid cancer.BMC Cancer. 2023 Sep 18;23(1):880. doi: 10.1186/s12885-023-11307-1. BMC Cancer. 2023. PMID: 37723469 Free PMC article.
References
-
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26:1–133. doi: 10.1089/thy.2015.0020. - DOI - PMC - PubMed
-
- Pedrazzini L, Baroli A, Marzoli L, Guglielmi R, Papini E. Cancer recurrence in papillary thyroid microcarcinoma: a multivariate analysis on 231 patients with a 12-year follow-up. Minerva Endocrinol. 2013;38:269–279. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
