

Early detection of T-cell lymphoma with T follicular helper phenotype by RHOA mutation analysis
- PMID: 33567811
- PMCID: PMC8804563
- DOI: 10.3324/haematol.2020.265991
Early detection of T-cell lymphoma with T follicular helper phenotype by RHOA mutation analysis
Abstract
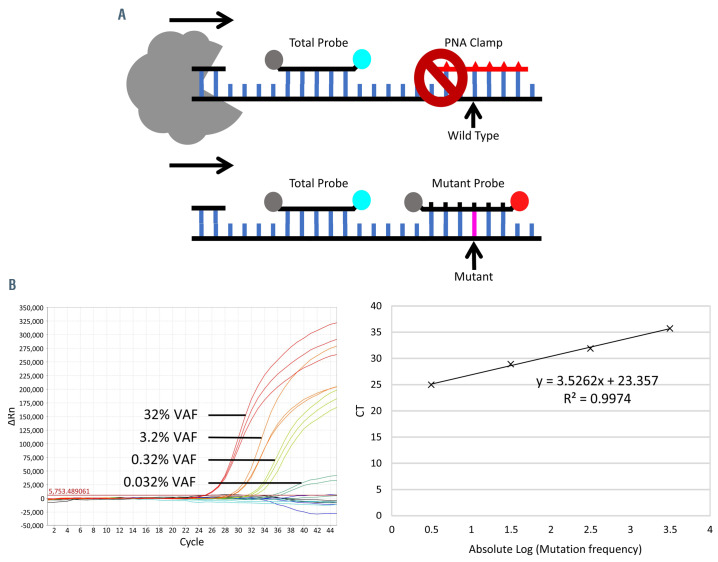
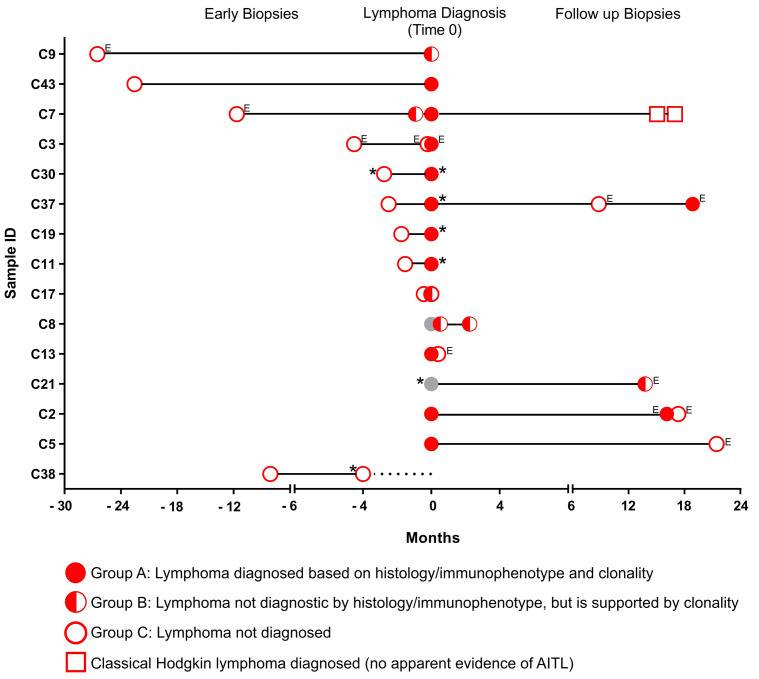
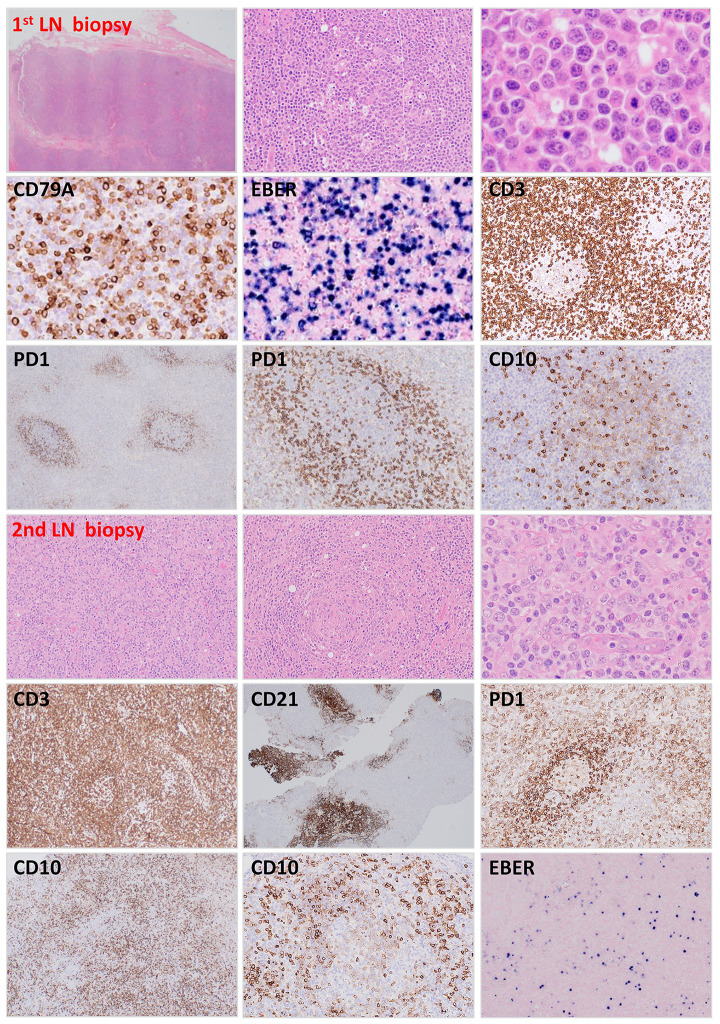
Angioimmunoblastic T-cell lymphoma (AITL) and peripheral T-cell lymphoma with T follicular helper phenotype (PTCL-TFH) are a group of complex clinicopathological entities that originate from T follicular helper cells and share a similar mutation profile. Their diagnosis is often a challenge, particularly at an early stage, because of a lack of specific histological and immunophenotypic features, paucity of neoplastic T cells and prominent polymorphous infiltrate. We investigated whether the lymphoma-associated RHOA Gly17Val (c.50G>T) mutation, occurring in 60% of cases, is present in the early "reactive" lesions, and whether mutation analysis could help to advance the early diagnosis of lymphoma. The RHOA mutation was detected by quantitative polymerase chain reaction with a locked nucleic acid probe specific to the mutation, and a further peptide nucleic acid clamp oligonucleotide to suppress the amplification of the wild-type allele. The quantitative polymerase chain reaction assay was highly sensitive and specific, detecting RHOA Gly17Val at an allele frequency of 0.03%, but not other changes in Gly17, nor in 61 controls. Among the 37 cases of AITL and PTCL-TFH investigated, RHOA Gly17Val was detected in 62.2% (23/37) of which 19 had multiple biopsies including preceding biopsies in ten and follow-up biopsies in 11 cases. RHOA Gly17Val was present in each of these preceding or follow-up biopsies including 18 specimens that showed no evidence of lymphoma by combined histological, immunophenotypic and clonality analyses. The mutation was seen in biopsies 0-26.5 months (mean 7.87 months) prior to the lymphoma diagnosis. Our results show that RHOA Gly17Val mutation analysis is valuable in the early detection of AITL and PTCL-TFH.
Figures

Similar articles
-
Droplet digital polymerase chain reaction assay and peptide nucleic acid-locked nucleic acid clamp method for RHOA mutation detection in angioimmunoblastic T-cell lymphoma.Cancer Sci. 2018 May;109(5):1682-1689. doi: 10.1111/cas.13557. Epub 2018 Mar 31. Cancer Sci. 2018. PMID: 29493850 Free PMC article.
-
Follicular Helper T-Cell-derived Nodal Lymphomas: Study of Histomorphologic, Immunophenotypic, Clinical, and RHOA G17V Mutational Profile.Appl Immunohistochem Mol Morphol. 2023 Mar 1;31(3):172-180. doi: 10.1097/PAI.0000000000001105. Epub 2023 Feb 20. Appl Immunohistochem Mol Morphol. 2023. PMID: 36806188
-
RHOA mutation in follicular T-cell lymphoma: Clinicopathological analysis of 16 cases.Pathol Int. 2020 Sep;70(9):653-660. doi: 10.1111/pin.12981. Epub 2020 Jul 9. Pathol Int. 2020. PMID: 32648273
-
Clinicopathological Implications of RHOA Mutations in Angioimmunoblastic T-Cell Lymphoma: A Meta-analysis: RHOA mutations in AITL.Clin Lymphoma Myeloma Leuk. 2021 Jul;21(7):431-438. doi: 10.1016/j.clml.2021.03.002. Epub 2021 Mar 19. Clin Lymphoma Myeloma Leuk. 2021. PMID: 33849798
-
[Diagnosis and treatment of angioimmunoblastic T-cell lymphoma and related cancers].Rinsho Ketsueki. 2019;60(9):1221-1228. doi: 10.11406/rinketsu.60.1221. Rinsho Ketsueki. 2019. PMID: 31597847 Review. Japanese.
Cited by
-
Genetic abnormalities assist in pathological diagnosis and EBV-positive cell density impact survival in Chinese angioimmunoblastic T-cell lymphoma patients.Chin J Cancer Res. 2023 Oct 30;35(5):536-549. doi: 10.21147/j.issn.1000-9604.2023.05.10. Chin J Cancer Res. 2023. PMID: 37969960 Free PMC article.
-
Precise diagnosis and targeted therapy of nodal T-follicular helper cell lymphoma (T-FHCL).Front Oncol. 2023 Apr 28;13:1163190. doi: 10.3389/fonc.2023.1163190. eCollection 2023. Front Oncol. 2023. PMID: 37188182 Free PMC article. Review.
-
Parallel evolution of two distinct lymphoid proliferations in clonal haematopoiesis.Histopathology. 2022 Apr;80(5):847-858. doi: 10.1111/his.14619. Epub 2022 Mar 1. Histopathology. 2022. PMID: 35064935 Free PMC article.
-
Primary cutaneous peripheral T-cell lymphomas with a T-follicular helper phenotype: an integrative clinical, pathological and molecular case series study.Br J Dermatol. 2022 Dec;187(6):970-980. doi: 10.1111/bjd.21791. Epub 2022 Sep 2. Br J Dermatol. 2022. PMID: 35895386 Free PMC article.
-
Molecular diagnosis of T-cell lymphoma: a correlative study of PCR-based T-cell clonality assessment and targeted NGS.Blood Adv. 2021 Nov 23;5(22):4590-4593. doi: 10.1182/bloodadvances.2021005249. Blood Adv. 2021. PMID: 34607351 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
