

Diagnostic accuracy of CBCT versus intraoral imaging for assessment of peri-implant bone defects
- PMID: 33568085
- PMCID: PMC7877020
- DOI: 10.1186/s12880-021-00557-9
Diagnostic accuracy of CBCT versus intraoral imaging for assessment of peri-implant bone defects
Abstract
Background: Early detection of marginal bone loss is vital for treatment planning and prognosis of teeth and implant. This study was conducted to assess diagnostic accuracy of CBCT compared to intra-oral (IO) radiography for detection, classification, and measurement of peri-implant bone defects in an animal model.
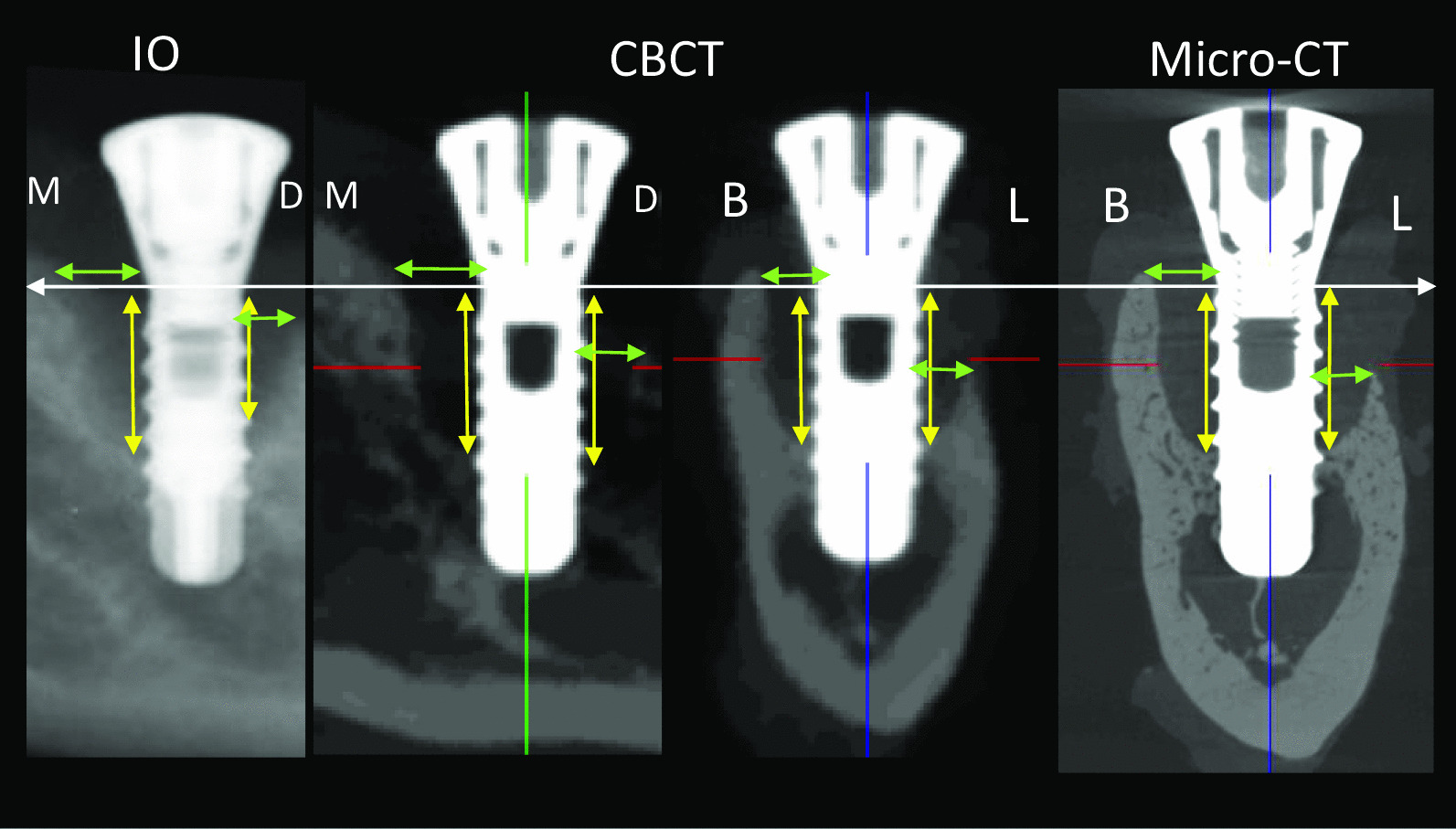
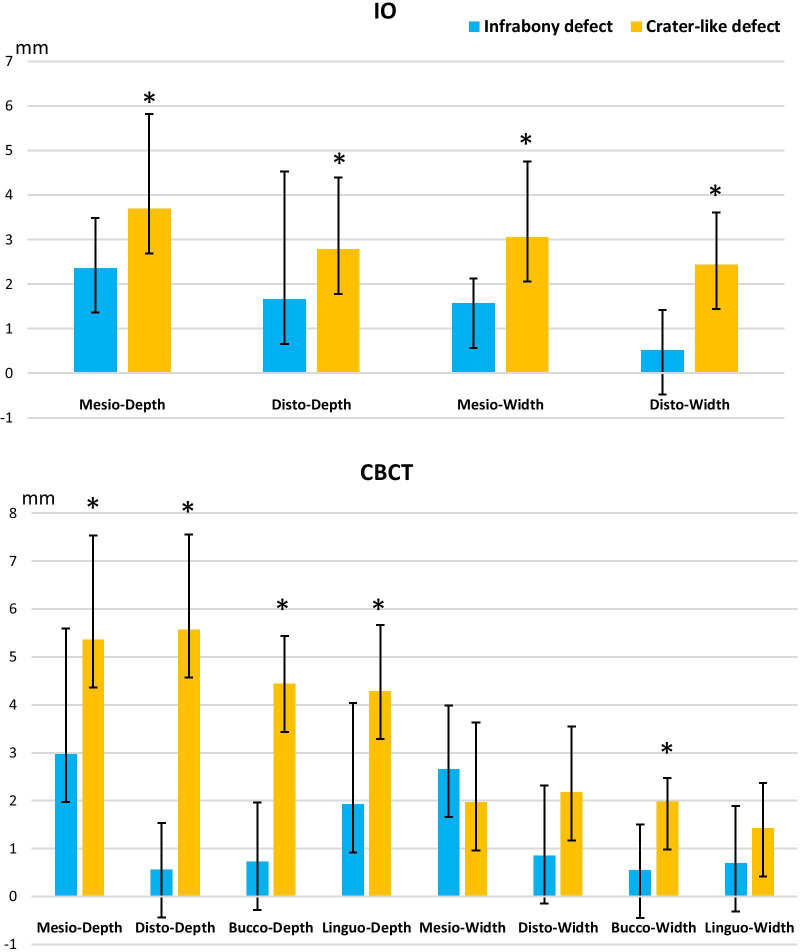
Methods: Fifty-four mandible blocks with implants were harvested from nine male health adult beagle dogs with acquisition of IO, CBCT and micro-CT images from all samples. Peri-implant bone defects from 16 samples were diagnosed using micro-CT and classified into 3 defect categories: dehiscence (n = 5), infrabony defect (n = 3) and crater-like defect (n = 8). Following training and calibration of the observers, they asked to detect location (mesial, distal, buccal, lingual) and shape of the defect (dehiscence, horizontal defect, vertical defect, carter-like defect) utilizing both IO and CBCT images. Both observers assessed defect depth and width on IO, CBCT and micro-CT images at each side of peri-implant bone defect via CT-analyzer software. Data were analyzed using SPSS software and a p value of < 0.05 was considered as statistically significant.
Results: Overall, there was a high diagnostic accuracy for detection of bone defects with CBCT images (sensitivity: 100%/100%), while IO images showed a reduction in accuracy (sensitivity: 69%/63%). Similarly, diagnostic accuracy for defect classification was significantly higher for CBCT, whereas IO images were unable to correctly identify vestibular dehiscence, with incorrect assessment of half of the infrabony defects. For accuracy of measuring defect depth and width, a higher correlation was observed between CBCT and gold standard micro-CT (r = 0.91, 95% CI 0.86-0.94), whereas a lower correlation was seen for IO images (r = 0.82, 95% CI 0.67-0.91).
Conclusions: The diagnostic accuracy and reliability of CBCT was found to be superior to IO imaging for the detection, classification, and measurement of peri-implant bone defects. The application of CBCT adds substantial information related to the peri-implant bone defect diagnosis and decision-making which cannot be achieved with conventional IO imaging.
Keywords: Alveolar bone loss; CBCT; Dental radiography; Peri‐implantitis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Harris D, Horner K, Gröndahl K, Jacobs R, Helmrot E, Benic GI, et al. E.A.O. guidelines for the use of diagnostic imaging in implant dentistry 2011. A consensus workshop organized by the European Association for Osseointegration at the Medical University of Warsaw. Clin Oral Implants Res. 2012;23:1243–53. doi: 10.1111/j.1600-0501.2012.02441.x. - DOI - PubMed
-
- Hilgenfeld T, Juerchott A, Deisenhofer UK, Krisam J, Rammelsberg P, Heiland S, et al. Accuracy of cone-beam computed tomography, dental magnetic resonance imaging, and intraoral radiography for detecting peri-implant bone defects at single zirconia implants---an in vitro study. Clin Oral Implants Res. 2018;29:922–30. doi: 10.1111/clr.13348. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
