

The Effects of Minimum Caseload Requirements on Management and Outcome in Abdominal Aortic Aneurysm Repair
- PMID: 33568259
- PMCID: PMC8005841
- DOI: 10.3238/arztebl.2020.0820
The Effects of Minimum Caseload Requirements on Management and Outcome in Abdominal Aortic Aneurysm Repair
Abstract
Background: The German quality assurance guideline on abdominal aortic aneurysm (AAA) was implemented by the Joint Federal Committee (Gemeinsamer Bundesausschuss, G-BA) in 2008. The aims of this study were to verify the association between hospital case volume and outcome and to assess the hypothetical effect of minimum caseload requirements.
Methods: The German diagnosis-related groups statistics for the years 2012 to 2016 were scrutinized for AAA (ICD-10 GM I71.3/4) with procedure codes for endo - vascular or open surgical treatment. The primary endpoint was in-hospital mortality. Logistic regression models were used for risk adjustment, and odds ratios (OR) were calculated as a function of the annual hospital-level case volume of AAA. In a hypo - thetical approach, the linear distances for various minimum caseloads (MC) were evaluated to assess accessibility.
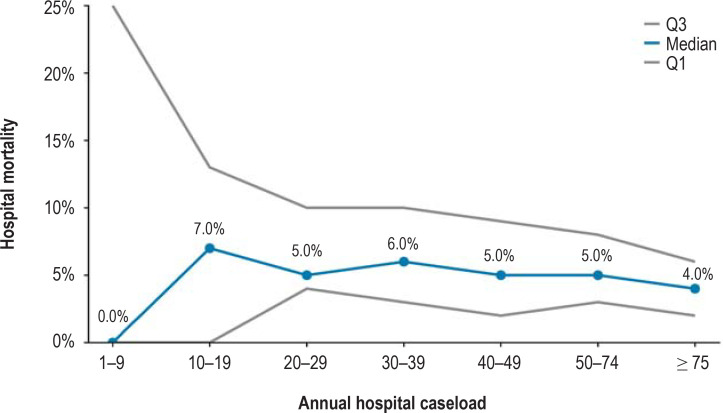
Results: The mortality of intact AAA (iAAA) was 2.7% (men [M] 2.4%, women [W] 4.2%); ruptured AAA (rAAA), 36.9% (M 36.9%, F 37.5%). An inverse relationship between annual hospital case volume of AAA and mortality was confirmed (iAAA/rAAA: from 3.9%/51% [<10 cases/year] through 3.3%/37% [30-39 cases/year] to 1.9%/28% [≥ 75 cases/year]). For a reference category of 30 AAA procedures/year, the following significant OR were found: 10 AAA cases/year, OR 1.21 (95% confidence interval [1.20; 1.21]); 20 cases, OR 1.09 [1.09; 1.09]; 50 cases, OR 0.89 [0.89; 0.89]; 75 cases, OR 0.82 [0.82; 0.82]. In a hypothetical centralization scenario with assumed MC of 30/year, 86% of the population would have to travel less than 100 km to the nearest hospital; with an MC of 40, this would apply to only 50% (without redistribution effects).
Conclusion: In the observed period, a significant correlation was confirmed between high annual case volume and low in-hospital mortality. A minimum caseload requirement of 30 AAA operations/year seems reasonable in view of the accessibility of hospitals. Cite this.
Figures






References
-
- Dueck AD, Kucey DS, Johnston KW, Alter D, Laupacis A. Survival after ruptured abdominal aortic aneurysm: effect of patient, surgeon, and hospital factors. J Vasc Surg. 2004;39:1253–1260. - PubMed
-
- Chaikof EL, Dalman RL, Eskandari MK, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018;67:2–77. - PubMed
-
- Debus ES, Heidemann F, Gross-Fengels W, et al. [Short version of the S3 guideline on screening, diagnosis, therapy and follow-up of abdominal aortic aneurysms] Gefasschirurgie. 2018;23:432–451.
MeSH terms
LinkOut - more resources
Full Text Sources