

Modified Dunn Osteotomy for Moderate and Severe Slipped Capital Femoral Epiphysis - A retrospective study of thirty hips
- PMID: 33569103
- PMCID: PMC7851261
- DOI: 10.1007/s43465-020-00156-w
Modified Dunn Osteotomy for Moderate and Severe Slipped Capital Femoral Epiphysis - A retrospective study of thirty hips
Abstract
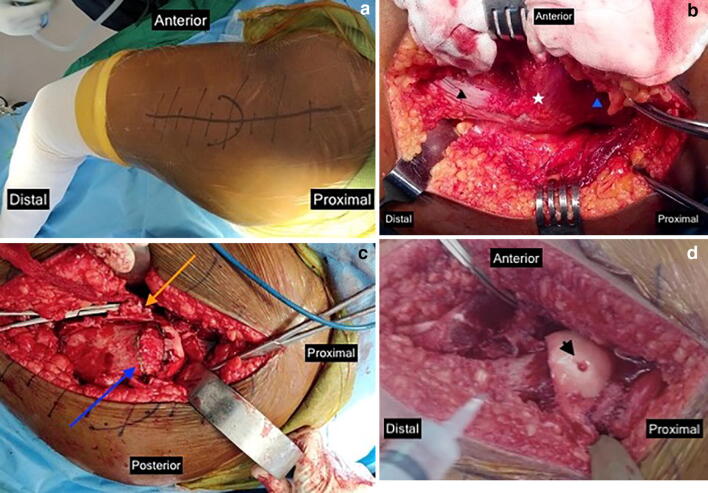
Background: Modified Dunn procedure has become popular for the treatment of severe cases of slipped capital femoral epiphysis (SCFE). We assessed the outcomes in a consecutive series of thirty Indian adolescents treated by the modified Dunn procedure.
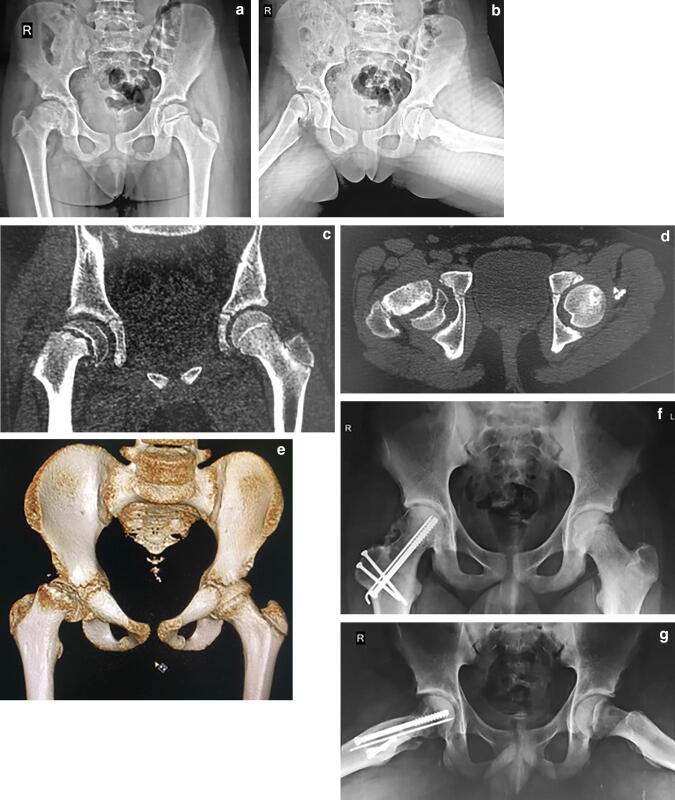
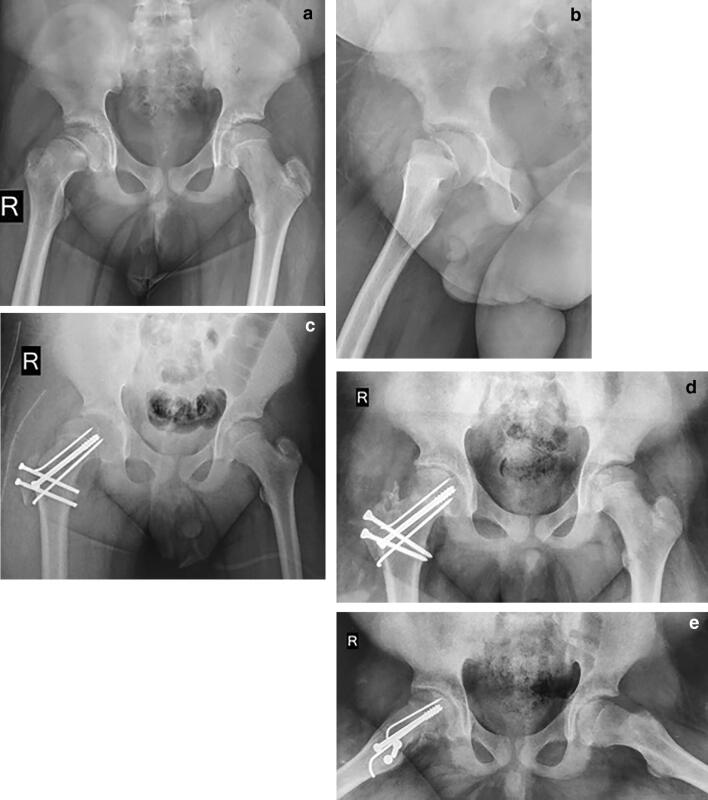
Materials and methods: All patients treated by the modified Dunn procedure by a single senior Paediatric Orthopaedic surgeon over six years were retrospectively reviewed. Only moderate and severe slips undergoing modified Dunn procedure were included. Clinical records and radiographs were reviewed to obtain demographic information; to classify the slips by duration of symptoms, severity and physeal stability; and to assess the outcomes by Harris Hip Score, radiological changes and rate of complications.
Results: Thirty consecutive hips with 19 stable and 11 unstable slips were included. Mean age was 13.05 years, 25 boys and 5 girls; six were acute slips, six chronic and eighteen acute-on-chronic. There were 20 moderate and 10 severe slips. Slip angle correction was on average 43.63° ± 8.42° (p < 0.001). At a mean follow-up of 25.36 months, the slip angle averaged 9.9° ± 3.78°, and alpha angle was 33.63° ± 4.14. The average Harris Hip Score was 81.833 ± 7.12 points, with six excellent, 17 good, six fair and one poor result. Osteonecrosis occurred in two hips (6.6%). One hip had post-operative subluxation which was corrected.
Conclusion: This study adds to the evidence that the modified Dunn procedure is safe, reliable and reproducible. It should be the first choice for the treatment of moderate and severe SCFE.
Keywords: Capital realignment; Indian adolescents; Modified dunn procedure; Safe surgical dislocation; Slipped capital femoral epiphysis.
© Indian Orthopaedics Association 2020.
Conflict of interest statement
Conflict of interestNone.
Figures
References
-
- Ross PM, Lyne ED, Morawa LG. Slipped capital femoral epiphysis long-term results after 10–38 years. Clinical Orthopaedics and Related Research. 1979;141:176–180. - PubMed
LinkOut - more resources
Full Text Sources