

Patient-Focused Selection of PrEP Medication for Individuals at Risk of HIV: A Narrative Review
- PMID: 33569743
- PMCID: PMC7875561
- DOI: 10.1007/s40121-020-00384-5
Patient-Focused Selection of PrEP Medication for Individuals at Risk of HIV: A Narrative Review
Abstract
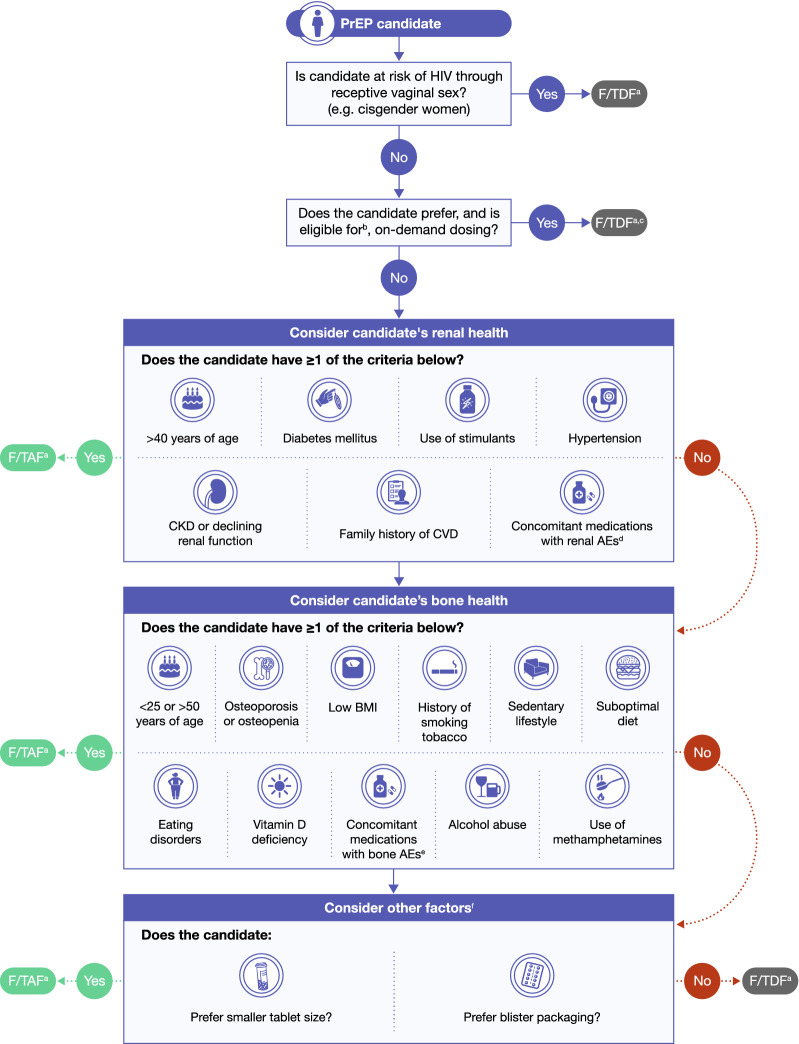
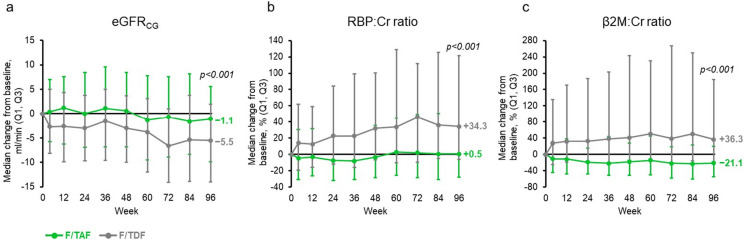
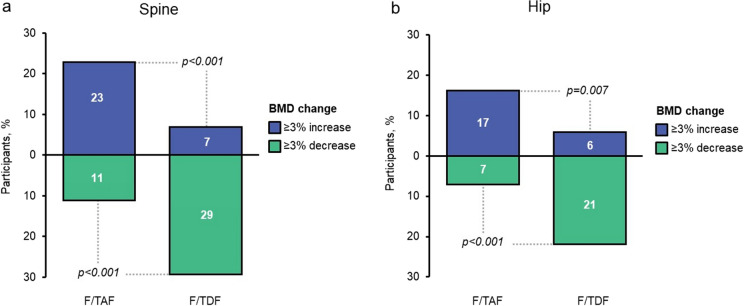
Pre-exposure prophylaxis (PrEP) medication is a key component of the HIV prevention strategy in the US, which has been demonstrated to be highly effective in preventing HIV acquisition among individuals at risk. Two PrEP medications are currently approved: emtricitabine/tenofovir disoproxil fumarate (Truvada®; F/TDF) was approved by the US Food and Drug Administration in 2012, followed by emtricitabine/tenofovir alafenamide (Descovy®; F/TAF) in 2019. An ongoing randomized, double-blind, Phase 3 study (DISCOVER) demonstrated that F/TAF had non-inferior efficacy to F/TDF. While both medications have been found to be efficacious and well tolerated, several studies have identified that important differences exist with regards to pharmacokinetics, bone and renal safety profiles, and other factors. In this narrative review, we conducted a comprehensive evaluation of the populations at risk of HIV who may also be affected by, or at risk of, bone or renal conditions. We reviewed the safety profiles of F/TDF and F/TAF to develop an evidence-based algorithm for selecting the appropriate PrEP medication, based on biological, behavioral, and health characteristics of an individual at risk of HIV, and considered how the choice of PrEP medication may or may not compound safety concerns for these individuals. We identified that the introduction of F/TAF provides a valuable alternative to F/TDF, allowing the personalization of PrEP. F/TAF may be the preferred medication for cisgender men and transgender women at risk of HIV infection who are predisposed to, or already have, bone or renal conditions. While the approval of F/TAF is the first step in personalization of PrEP, additional options are still warranted to help accommodate the wide spectrum of individuals at risk of HIV with different lifestyles, medical histories, preferences, and requirements.
Keywords: Bone; Decision making; HIV prevention; Kidney; Personalized medicine; Pre-exposure prophylaxis; Preference; Renal; Tenofovir alafenamide; Tenofovir disoproxil fumarate.
Plain language summary
Pre-exposure prophylaxis (or PrEP) prevents HIV acquisition in individuals at risk of HIV infection. There are currently two approved options for PrEP in the US; both are oral medications. The first option, approved in 2012, is a combination of two drugs called emtricitabine/tenofovir disoproxil fumarate—also known as Truvada® or F/TDF. The second option, approved in 2019, is a combination of emtricitabine and a different prodrug, tenofovir alafenamide—this combination is called Descovy® or F/TAF. Both options are 99% effective in preventing HIV if taken daily. While the risk of serious side effects from taking either of the PrEP medications is low, F/TAF has demonstrated less effect on bone and kidney health, and may be the preferred option in people with bone or kidney conditions, or in those at risk of developing osteoporosis or having risk factors for kidney disease, such as people living with diabetes or high blood pressure. As the risk of HIV sometimes overlaps with risks to bone and renal health according to race/ethnicity, poverty, alcohol/substance use, smoking tobacco, and taking other medications, F/TAF as an alternative PrEP medication allows the PrEP choice to depend on the broader health conditions of the individual. ‘Personalized medicine’ means that medicines can be chosen to suit an individual’s biology, behavior, lifestyle, and overall health. The approval of F/TAF is the first step in personalization of PrEP medication, while additional options need to be researched to meet the requirements of all individuals at risk of HIV.
Figures
References
-
- Centers for Disease Control and Prevention. HIV surveillance report, 2018 (updated); vol. 31. 2020. https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveil.... Accessed 23 Sept 2020.
-
- HIV.gov. What is ending the HIV epidemic: a plan for America. 2020. https://www.hiv.gov/federal-response/ending-the-hiv-epidemic/overview. Accessed 23 Sept 2020.
-
- Khalili J, Landovitz RJ. HIV preexposure prophylaxis—the role of primary care clinicians in ending the HIV epidemic. JAMA Intern Med. 2020;180:126–130. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
