

Population-Based Prostate Cancer Screening With Magnetic Resonance Imaging or Ultrasonography: The IP1-PROSTAGRAM Study
- PMID: 33570542
- PMCID: PMC7879388
- DOI: 10.1001/jamaoncol.2020.7456
Population-Based Prostate Cancer Screening With Magnetic Resonance Imaging or Ultrasonography: The IP1-PROSTAGRAM Study
Abstract
Importance: Screening for prostate cancer using prostate-specific antigen (PSA) testing can lead to problems of underdiagnosis and overdiagnosis. Short, noncontrast magnetic resonance imaging (MRI) or transrectal ultrasonography might overcome these limitations.
Objective: To compare the performance of PSA testing, MRI, and ultrasonography as screening tests for prostate cancer.
Design, setting, and participants: This prospective, population-based, blinded cohort study was conducted at 7 primary care practices and 2 imaging centers in the United Kingdom. Men 50 to 69 years of age were invited for prostate cancer screening from October 10, 2018, to May 15, 2019.
Interventions: All participants underwent screening with a PSA test, MRI (T2 weighted and diffusion), and ultrasonography (B-mode and shear wave elastography). The tests were independently interpreted without knowledge of other results. Both imaging tests were reported on a validated 5-point scale of suspicion. If any test result was positive, a systematic 12-core biopsy was performed. Additional image fusion-targeted biopsies were performed if the MRI or ultrasonography results were positive.
Main outcomes and measures: The main outcome was the proportion of men with positive MRI or ultrasonography (defined as a score of 3-5 or 4-5) or PSA test (defined as PSA ≥3 μg/L) results. Key secondary outcomes were the number of clinically significant and clinically insignificant cancers detected if each test was used exclusively. Clinically significant cancer was defined as any Gleason score of 3+4 or higher.
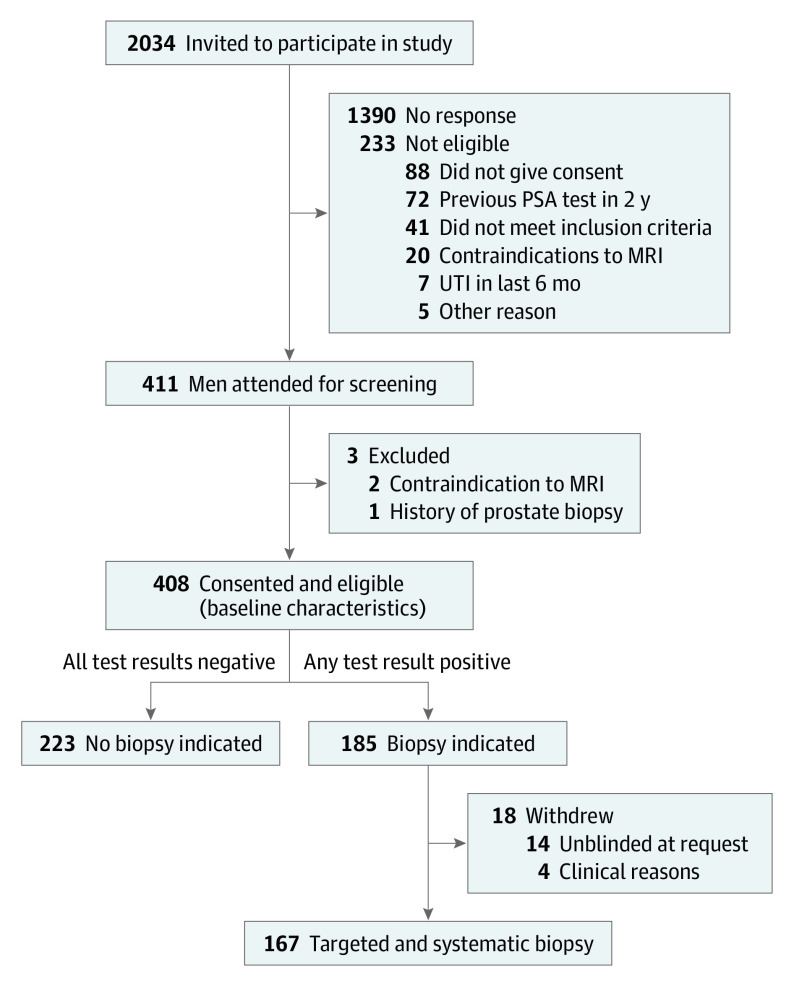
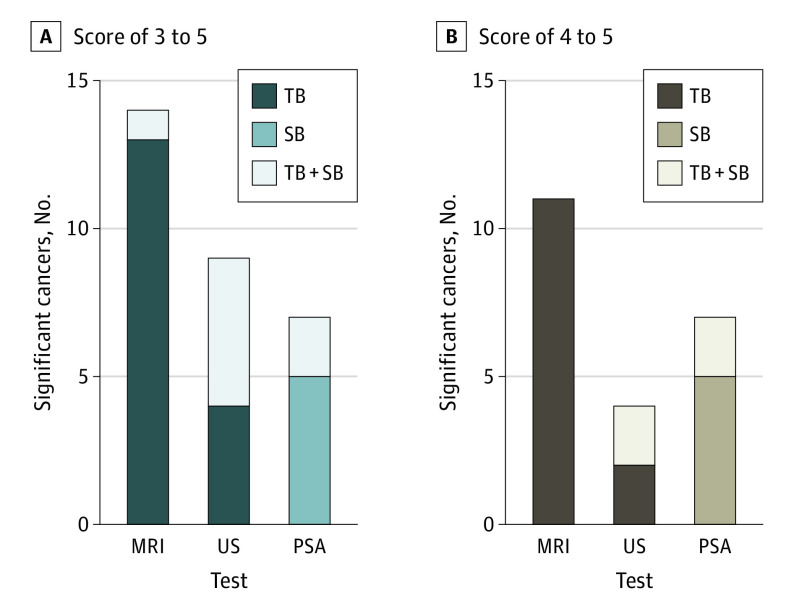
Results: A total of 2034 men were invited to participate; of 411 who attended screening, 408 consented to receive all screening tests. The proportion with positive MRI results (score, 3-5) was higher than the proportion with positive PSA test results (72 [17.7%; 95% CI, 14.3%-21.8%] vs 40 [9.9%; 95% CI, 7.3%-13.2%]; P < .001). The proportion with positive ultrasonography results (score, 3-5) was also higher than the proportion of those with positive PSA test results (96 [23.7%; 95% CI, 19.8%-28.1%]; P < .001). For an imaging threshold of score 4 to 5, the proportion with positive MRI results was similar to the proportion with positive PSA test results (43 [10.6%; 95% CI, 7.9%-14.0%]; P = .71), as was the proportion with positive ultrasonography results (52 [12.8%; 95% CI, 9.9%-16.5%]; P = .15). The PSA test (≥3 ng/mL) detected 7 clinically significant cancers, an MRI score of 3 to 5 detected 14 cancers, an MRI score of 4 to 5 detected 11 cancers, an ultrasonography score of 3 to 5 detected 9 cancer, and an ultrasonography score of 4 to 5 detected 4 cancers. Clinically insignificant cancers were diagnosed by PSA testing in 6 cases, by an MRI score of 3 to 5 in 7 cases, an MRI score of 4 to 5 in 5 cases, an ultrasonography score of 3 to 5 in 13 cases, and an ultrasonography score of 4 to 5 in 7 cases.
Conclusions and relevance: In this cohort study, when screening the general population for prostate cancer, MRI using a score of 4 or 5 to define a positive test result compared with PSA alone at 3 ng/mL or higher was associated with more men diagnosed with clinically significant cancer, without an increase in the number of men advised to undergo biopsy or overdiagnosed with clinically insignificant cancer. There was no evidence that ultrasonography would have better performance compared with PSA testing alone.
Conflict of interest statement
Figures
Comment in
-
Community-Based Screening for Prostate Cancer: A Role for Magnetic Resonance Imaging?JAMA Oncol. 2021 Mar 1;7(3):402-403. doi: 10.1001/jamaoncol.2020.7294. JAMA Oncol. 2021. PMID: 33570559 No abstract available.
-
Urological Oncology: Prostate Cancer.J Urol. 2021 Jul;206(1):158-161. doi: 10.1097/JU.0000000000001814. Epub 2021 Apr 21. J Urol. 2021. PMID: 33881346 No abstract available.
-
Beyond the AJR: "Population-Based Prostate Cancer Screening With Magnetic Resonance Imaging or Ultrasonography: The IP1-PROSTAGRAM Study".AJR Am J Roentgenol. 2021 Dec;217(6):1481. doi: 10.2214/AJR.21.26048. Epub 2021 Apr 28. AJR Am J Roentgenol. 2021. PMID: 33908267 No abstract available.
-
Population-Based Prostate Cancer Screening With Magnetic Resonance Imaging or Ultrasonography-The IP1-PROSTAGRAM Study.JAMA Oncol. 2021 Oct 1;7(10):1575. doi: 10.1001/jamaoncol.2021.2964. JAMA Oncol. 2021. PMID: 34410313 No abstract available.
-
Population-Based Prostate Cancer Screening With Magnetic Resonance Imaging or Ultrasonography-The IP1-PROSTAGRAM Study-Reply.JAMA Oncol. 2021 Oct 1;7(10):1575-1576. doi: 10.1001/jamaoncol.2021.2967. JAMA Oncol. 2021. PMID: 34410324 No abstract available.
References
-
- US Preventive Services Task Force . Final Recommendation Statement: Prostate Cancer: Screening. May 2018. Accessed February 29, 2020. https://www.uspreventiveservicestaskforce.org/uspstf/document/Recommenda...
-
- UK National Screening Committee (NSC) . The UK NSC Recommendation on Prostate Cancer Screening/PSA Testing in Men Over the Age of 50. Accessed February 29, 2020. https://legacyscreening.phe.org.uk/prostatecancer
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
