

A pragmatic multi-institutional approach to understanding transplant-associated thrombotic microangiopathy after stem cell transplant
- PMID: 33570619
- PMCID: PMC7805323
- DOI: 10.1182/bloodadvances.2020003455
A pragmatic multi-institutional approach to understanding transplant-associated thrombotic microangiopathy after stem cell transplant
Abstract
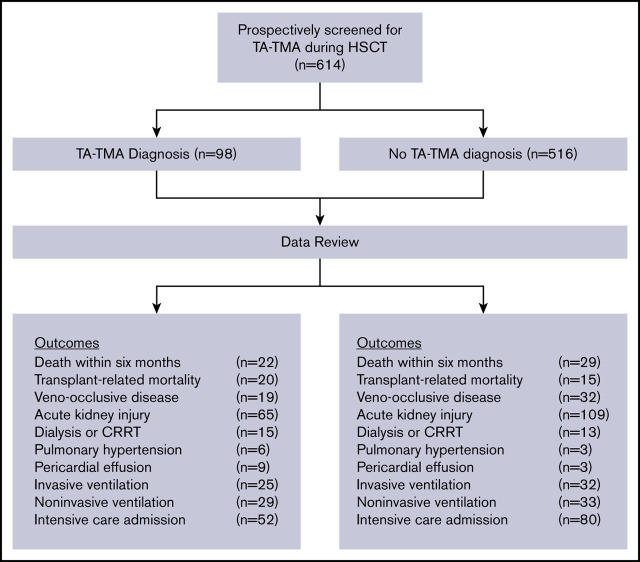
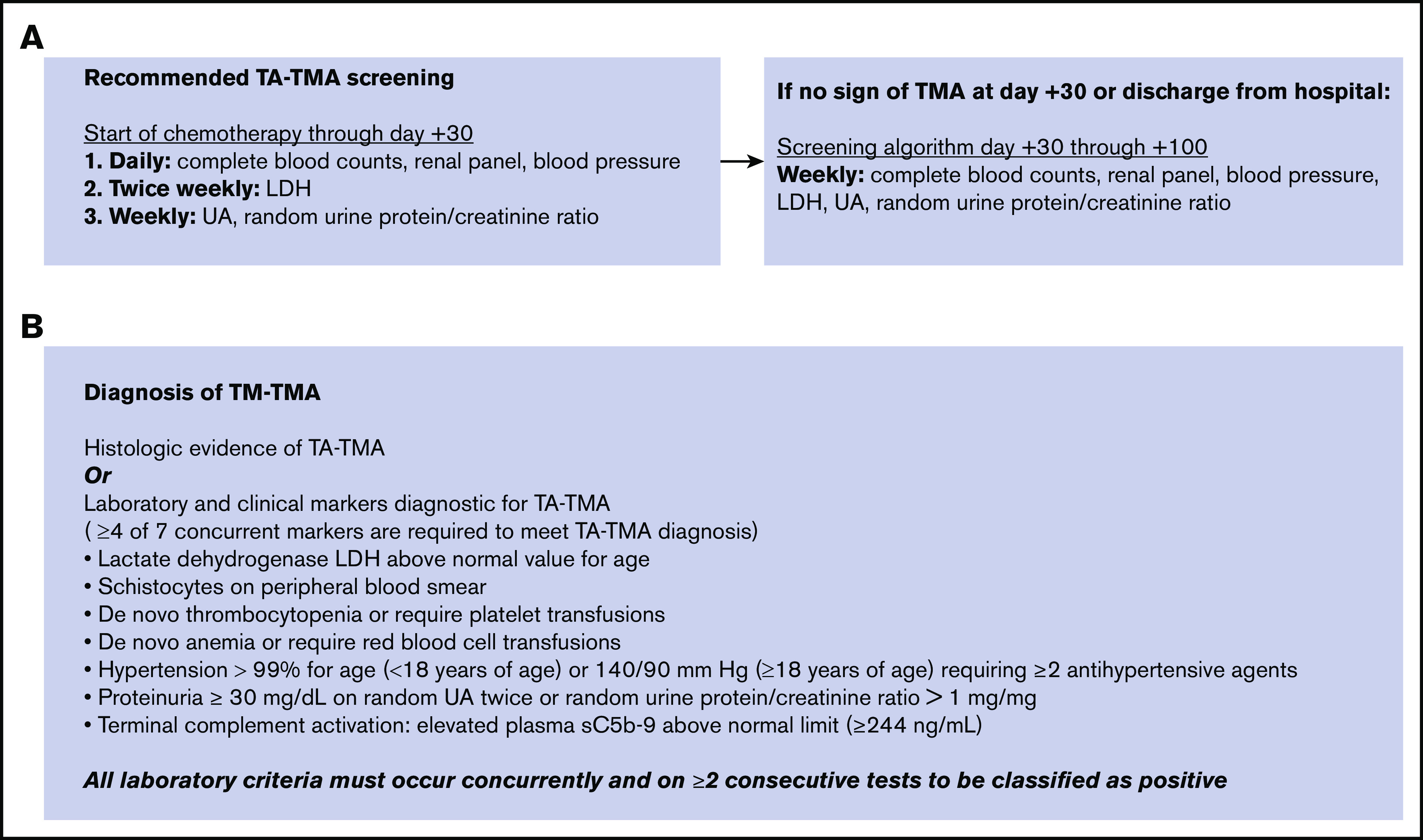
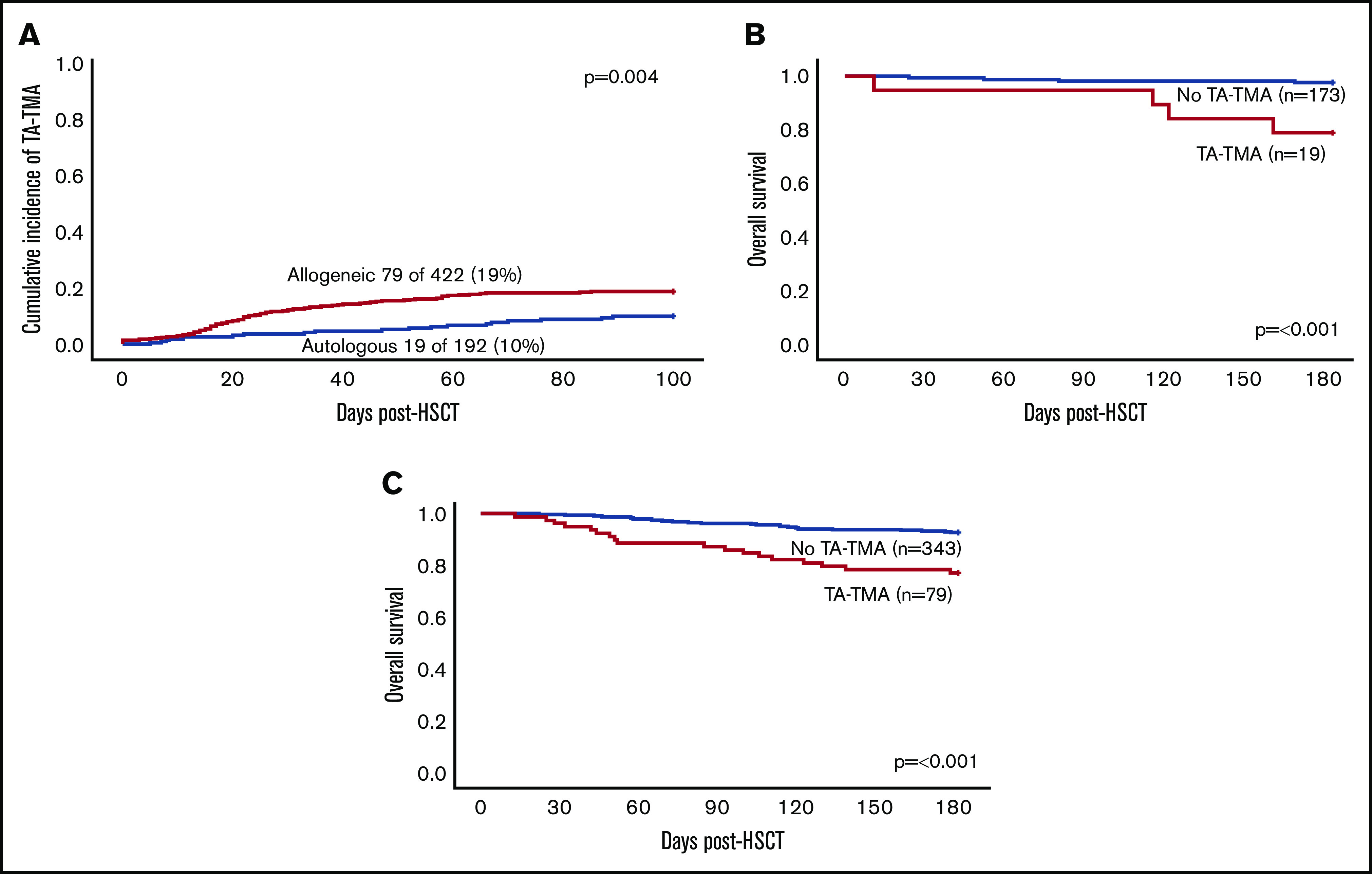
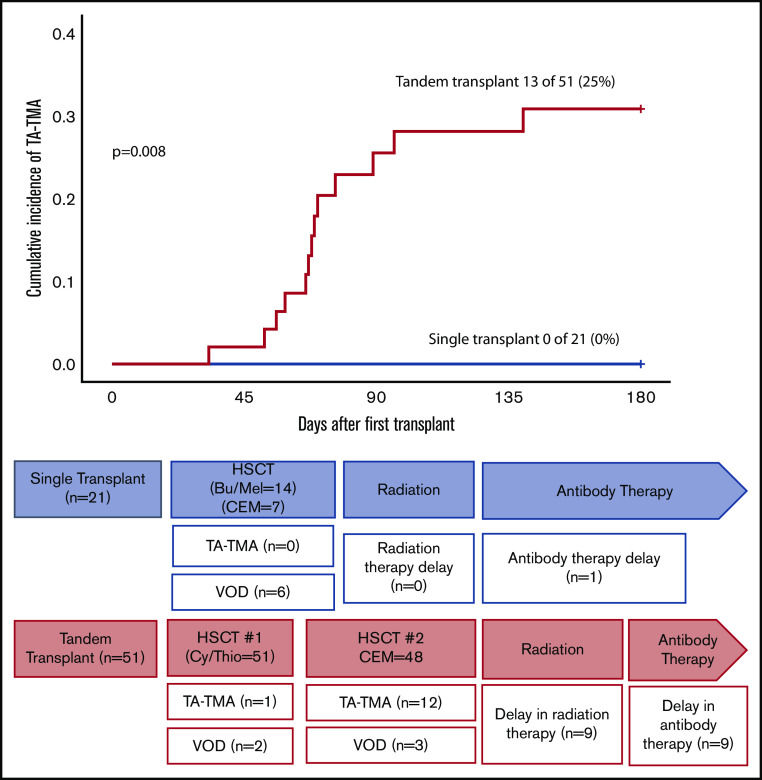
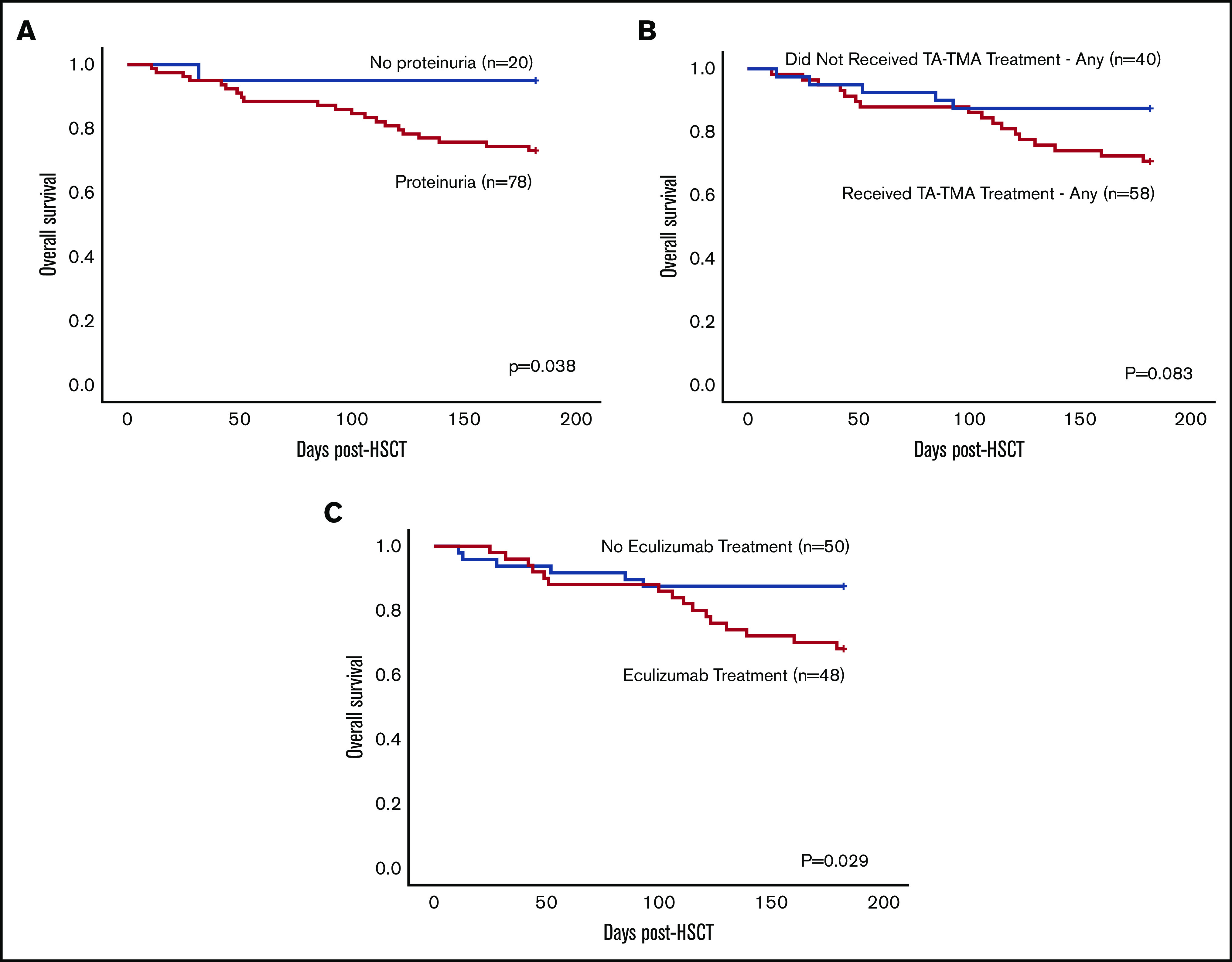
Transplant-associated thrombotic microangiopathy (TA-TMA) is a severe complication of hematopoietic stem cell transplantation (HSCT). A single-center prospective screening study has shown that the incidence of TA-TMA is much higher than prior retrospective studies that did not systematically screen. These data have not been replicated in a multicenter study. Our objective was to determine the incidence and risk factors for TA-TMA and compare outcomes of pediatric HSCT patients with and without TA-TMA. Patients were prospectively screened for TA-TMA at participating centers using a simple to implement and inexpensive strategy from the start of the preparative regimen through day +100. TA-TMA was diagnosed if ≥4 of 7 laboratory/clinical markers diagnostic for TA-TMA were present concurrently or if tissue histology showed TA-TMA. A total of 614 patients (359 males; 58%) received prospective TA-TMA screening at 13 pediatric centers. TA-TMA was diagnosed in 98 patients (16%) at a median of 22 days (interquartile range, 14-44) posttransplant. Patients with TA-TMA had significantly increased bloodstream infections (38% [37/98] vs 21% [107/51], P ≤ .001), mean total hospitalization days (68; 95% confidence interval [CI], 63-74 vs 43; 95% CI, 41-45; P ≤ .001), and number of days spent in the intensive care unit (10.1; 95% CI, 6.4-14; vs 1.6; 95% CI, 1.1-2.2; P ≤ .001) in the first 100 days after HSCT compared with patients without TA-TMA. Overall survival was significantly higher in patients without TA-TMA (93%; 490/516) compared with patients with TA-TMA (78%; 76/98) (P ≤ .001). These data support the need for systematic screening for TA-TMA and demonstrate the feasibility and efficacy of an easy to implement strategy to do so.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: C.C.D. has acted as a consultant for Alexion, Inc. and Omeros Corporation. C.E.D. has received travel support and honoraria for lectures at European Society for Blood and Marrow Transplantation (EBMT) and American Society of Transplantation and Cellular Therapy (ASTCT) meetings from Omeros. P.R. has served as a member of the speaker;s bureau for Sobi. R.P. has served on the advisory board for Orchard Therapeutics. S.J. has US patent applications under review, is a lead Principal Investigator for a National Institutes of Health–funded multi-institutional study with drug provided by Alexion Pharmaceuticals, and has received travel support and honoraria for lectures at EBMT and ASTCT meetings from Omeros. S.M.D. has acted as a consultant for Novartis and has research support from Alexion Pharmaceuticals. The remaining authors declare no competing financial interests.
Figures

References
-
- Barriga F, Ramírez P, Wietstruck A, Rojas N. Hematopoietic stem cell transplantation: clinical use and perspectives. Biol Res. 2012;45(3):307-316. - PubMed
-
- Copelan EA. Hematopoietic stem-cell transplantation. N Engl J Med. 2006;354(17):1813-1826. - PubMed
-
- Remberger M, Ackefors M, Berglund S, et al. . Improved survival after allogeneic hematopoietic stem cell transplantation in recent years. A single-center study. Biol Blood Marrow Transplant. 2011;17(11):1688-1697. - PubMed
-
- Dandoy CE, Jodele S, Paff Z, et al. . Team-based approach to identify cardiac toxicity in critically ill hematopoietic stem cell transplant recipients. Pediatr Blood Cancer. 2017;64(10):e26513. - PubMed
