

Preemptive ganciclovir for mechanically ventilated patients with cytomegalovirus reactivation
- PMID: 33570708
- PMCID: PMC7876264
- DOI: 10.1186/s13613-020-00793-2
Preemptive ganciclovir for mechanically ventilated patients with cytomegalovirus reactivation
Abstract
Background: The effect of cytomegalovirus (CMV) reactivation on the length of mechanical ventilation and mortality in immunocompetent ICU patients requiring invasive mechanical ventilation remains controversial. The main objective of this study was to determine whether preemptive intravenous ganciclovir increases the number of ventilator-free days in patients with CMV blood reactivation.
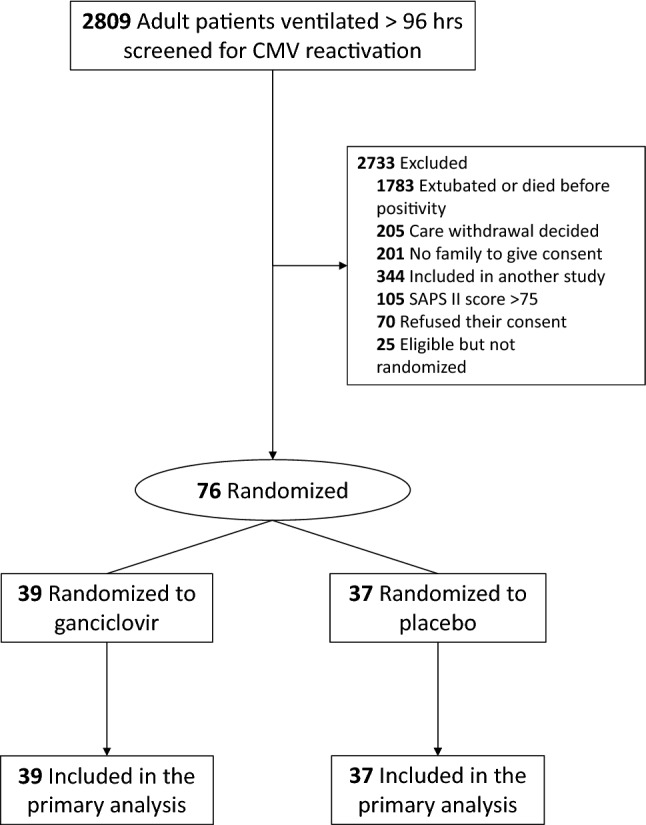
Methods: This double-blind, placebo-controlled, randomized clinical trial involved 19 ICUs in France. Seventy-six adults ≥ 18 years old who had been mechanically ventilated for at least 96 h, expected to remain on mechanical ventilation for ≥ 48 h, and exhibited reactivation of CMV in blood were enrolled between February 5th, 2014, and January 23rd, 2019. Participants were randomized to receive ganciclovir 5 mg/kg bid for 14 days (n = 39) or a matching placebo (n = 37).
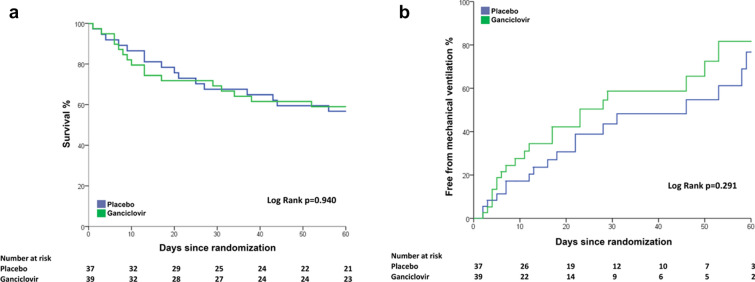
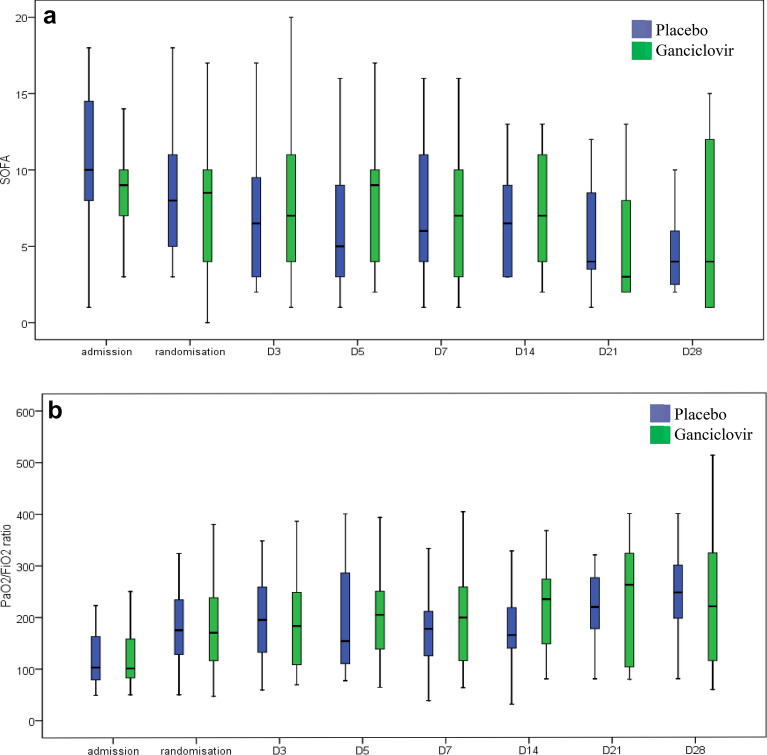
Results: The primary endpoint was ventilator-free days from randomization to day 60. Prespecified secondary outcomes included day 60 mortality. The trial was stopped for futility based on the results of an interim analysis by the DSMB. The subdistribution hazard ratio for being alive and weaned from mechanical ventilation at day 60 for patients receiving ganciclovir (N = 39) compared with control patients (N = 37) was 1.14 (95% CI from 0.63 to 2.06; P = 0.66). The median [IQR] numbers of ventilator-free days for ganciclovir-treated patients and controls were 10 [0-51] and 0 [0-43] days, respectively (P = 0.46). Mortality at day 60 was 41% in patients in the ganciclovir group and 43% in the placebo group (P = .845). Creatinine levels and blood cells counts did not differ significantly between the two groups.
Conclusions: In patients mechanically ventilated for ≥ 96 h with CMV reactivation in blood, preemptive ganciclovir did not improve the outcome.
Keywords: Clinical trial; Immunocompetent; Mechanical ventilation; Mortality; Randomized.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported. The following conflicts of interest are outside the area of the article. Dr Papazian reports receiving lecture fees from Hamilton. Dr Jaber reports receiving consulting fees from Dräger, Fisher-Paykel, Xenios-Fresenius Medical and Medtronic. Dr Aissaoui reports receiving lecture fees from Astra-Zeneca and Thoratec. Dr Lu reports receiving lectures fees from Aerogen. Dr Chastre reports receiving lecture and consulting fees from Bayer Healthcare, Pfizer, Merck Sharp & Dohme, Aridis, the Medicines Company, Astra Zeneca, Tigenix, Accelerate Diagnotics, Inotrem and Glaxo Smith Kline. Dr Luyt reports receiving lecture fees from ThermoFisher Brahms, Biomérieux, Merck Sharp & Dohme and Aerogen, and consulting fees from Bayer Healthcare, Carmat and Faron. Dr Leone reports receiving fees for lectures from MSD, Pfizer, Octapharma, 3M, Biomérieux and for consulting from Amomed, Aguettant and Gilead. Dr Chastre has received honoraria for lectures, or for participating in advisory boards, from Accelerate Diagnostics, AstraZeneca/Medimmune, Bayer, Cubist/Merck, GSK, Inotrem, Kenta/Aridis, Shionogi and Tigenix.
Figures
References
-
- Gkrania-Klotsas E, Langenberg C, Sharp SJ, Luben R, Khaw KT, Wareham NJ. Higher immunoglobulin G antibody levels against cytomegalovirus are associated with incident ischemic heart disease in the population-based EPIC-Norfolk cohort. J Infect Dis. 2012;206(12):1897–1903. doi: 10.1093/infdis/jis620. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
