

Dual inhibition of TGFβ and AXL as a novel therapy for human colorectal adenocarcinoma with mesenchymal phenotype
- PMID: 33570712
- PMCID: PMC7878213
- DOI: 10.1007/s12032-021-01464-3
Dual inhibition of TGFβ and AXL as a novel therapy for human colorectal adenocarcinoma with mesenchymal phenotype
Abstract
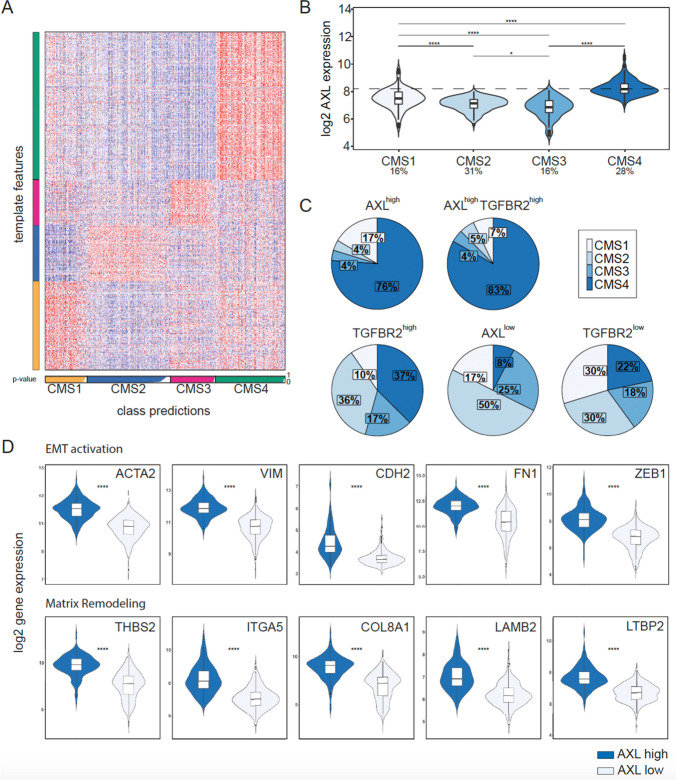
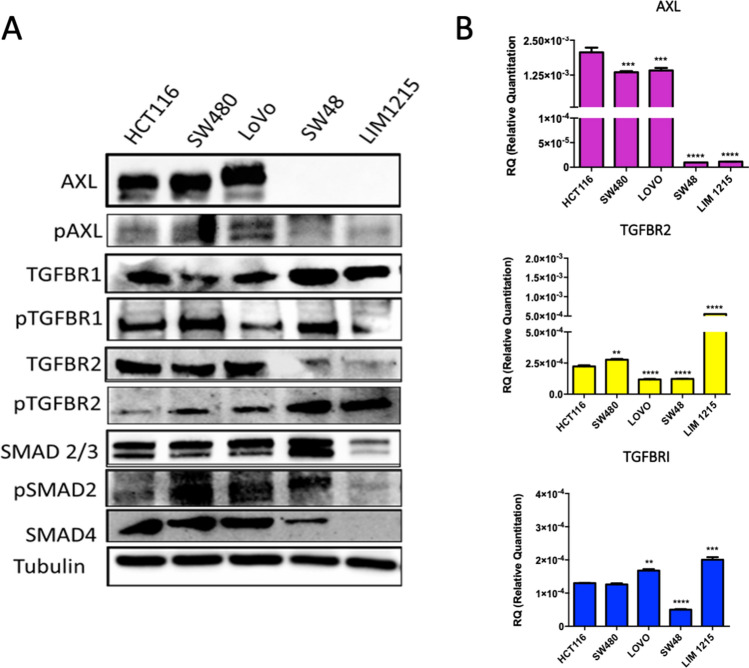
A subset of colorectal cancer (CRC) with a mesenchymal phenotype (CMS4) displays an aggressive disease, with an increased risk of recurrence after surgery, reduced survival, and resistance to standard treatments. It has been shown that the AXL and TGFβ signaling pathways are involved in epithelial-to-mesenchymal transition, migration, metastatic spread, and unresponsiveness to targeted therapies. However, the prognostic role of the combination of these biomarkers and the anti-tumor effect of AXL and TGFβ inhibition in CRC still has to be assessed. To evaluate the role of AXL and TGFβ as negative biomarker in CRC, we conducted an in-depth in silico analysis of CRC samples derived from the Gene Expression Omnibus. We found that AXL and TGFβ receptors are upregulated in CMS4 tumors and are correlated with an increased risk of recurrence after surgery in stage II/III CRC and a reduced overall survival. Moreover, we showed that AXL receptor is differently expressed in human CRC cell lines. Dual treatment with the TGFβ galunisertib and the AXL inhibitor, bemcentinib, significantly reduced colony formation and migration capabilities of tumor cells and displayed a strong anti-tumor activity in 3D spheroid cultures derived from patients with advanced CRC. Our work shows that AXL and TGFβ receptors identify a subgroup of CRC with a mesenchymal phenotype and correlate with poor prognosis. Dual inhibition of AXL and TGFβ could represent a novel therapeutic strategy for patients with this aggressive disease.
Keywords: AXL; Colorectal cancer; EMT; TGFβ.
Conflict of interest statement
DC reports travel grant from Sanofi; FM: Advisory Boards: MSD, Lilly; Institutional Research Grants: AstraZeneca; TT reports advisory board for Amgen, Bayer, Merck, Novartis, Roche, Sanofi; FC reports advisory board for Merck, Roche, Amgen, Bayer, Servier, Symphogen, Pfizer and research funding from Roche, Merck, Amgen, Bayer, Ipsen; EM advisory board for Amgen, Bayer, Merck, Roche, Sanofi, Servier and expert opinion for ESMO (European Society of Medical Oncology); all the other authors reports no conflict of interest.
Figures



References
-
- Howlader N, Noone AM, Krapcho M, et al (eds). SEER Cancer Statistics Review, 1975–2016, National Cancer Institute, Bethesda, MD, https://seer.cancer.gov/csr/1975_2016/, based on November 2018 SEER data submission, posted to the SEER website, April 2019.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
