

A Machine Learning Approach Enables Quantitative Measurement of Liver Histology and Disease Monitoring in NASH
- PMID: 33570776
- PMCID: PMC8361999
- DOI: 10.1002/hep.31750
A Machine Learning Approach Enables Quantitative Measurement of Liver Histology and Disease Monitoring in NASH
Abstract
Background and aims: Manual histological assessment is currently the accepted standard for diagnosing and monitoring disease progression in NASH, but is limited by variability in interpretation and insensitivity to change. Thus, there is a critical need for improved tools to assess liver pathology in order to risk stratify NASH patients and monitor treatment response.
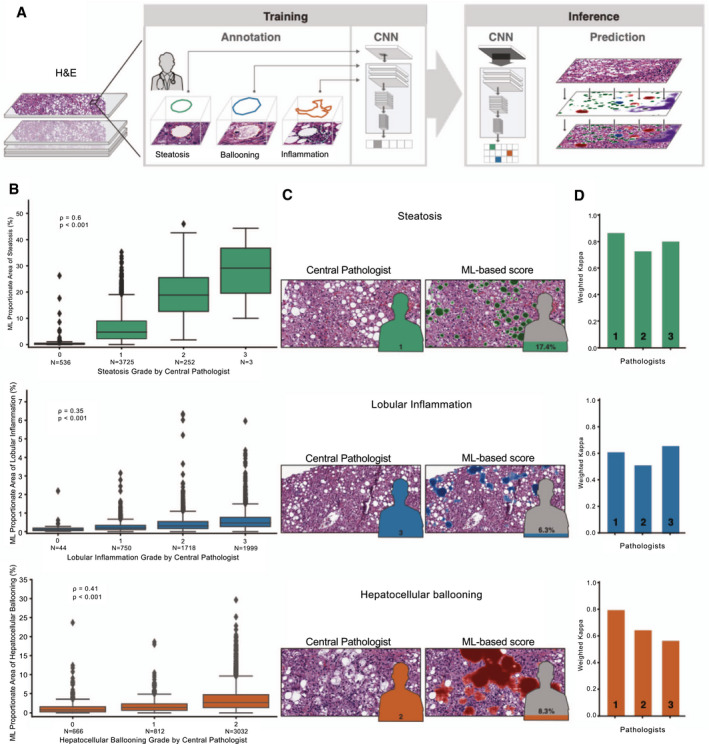
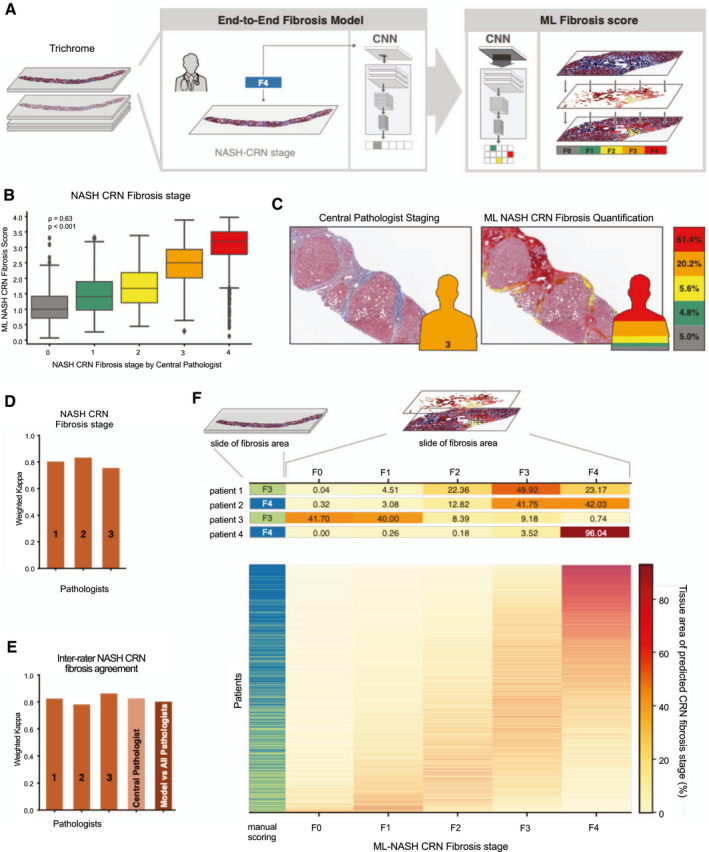
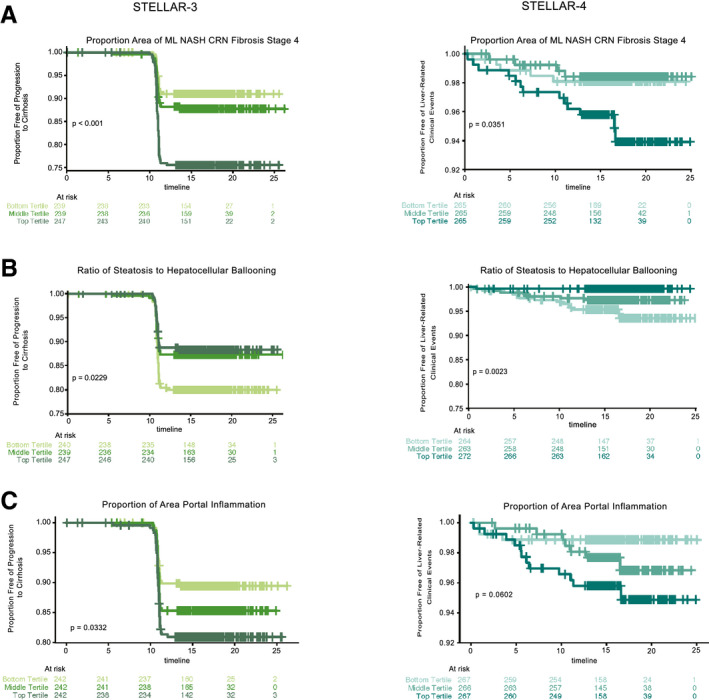
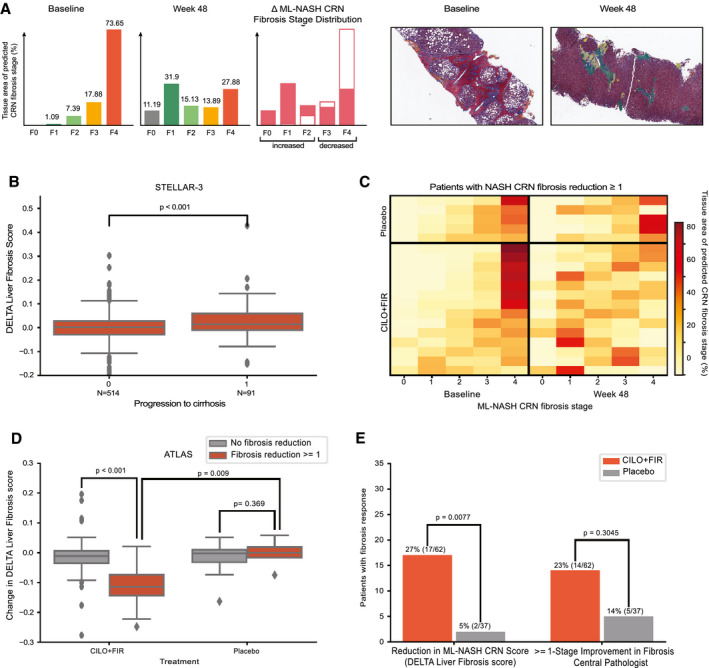
Approach and results: Here, we describe a machine learning (ML)-based approach to liver histology assessment, which accurately characterizes disease severity and heterogeneity, and sensitively quantifies treatment response in NASH. We use samples from three randomized controlled trials to build and then validate deep convolutional neural networks to measure key histological features in NASH, including steatosis, inflammation, hepatocellular ballooning, and fibrosis. The ML-based predictions showed strong correlations with expert pathologists and were prognostic of progression to cirrhosis and liver-related clinical events. We developed a heterogeneity-sensitive metric of fibrosis response, the Deep Learning Treatment Assessment Liver Fibrosis score, which measured antifibrotic treatment effects that went undetected by manual pathological staging and was concordant with histological disease progression.
Conclusions: Our ML method has shown reproducibility and sensitivity and was prognostic for disease progression, demonstrating the power of ML to advance our understanding of disease heterogeneity in NASH, risk stratify affected patients, and facilitate the development of therapies.
© 2021 PathAI. Hepatology published by Wiley Periodicals LLC on behalf of American Association for the Study of Liver Diseases.
Figures
Comment in
-
Artificial Intelligence in NASH Histology: Human Teaches a Machine for the Machine to Help Humans.Hepatology. 2021 Jul;74(1):9-11. doi: 10.1002/hep.31777. Epub 2021 May 22. Hepatology. 2021. PMID: 33638172 No abstract available.
References
-
- Estes C, Anstee QM, Arias‐Loste MT, Bantel H, Bellentani S, Caballeria J, et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016‐2030. J Hepatol 2018;69:896‐904. - PubMed
-
- Younossi Z, Stepanova M, Ong JP, Jacobson IM, Bugianesi E, Duseja A, et al. Nonalcoholic steatohepatitis is the fastest growing cause of hepatocellular carcinoma in liver transplant candidates. Clin Gastroenterol Hepatol 2019;17:748‐755.e3. - PubMed
-
- Kleiner DE, Brunt EM, Van Natta M, Behling C, Contos MJ, Cummings OW, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005;41:1313‐1321. - PubMed
-
- Merriman RB, Ferrell LD, Patti MG, Weston SR, Pabst MS, Aouizerat BE, et al. Correlation of paired liver biopsies in morbidly obese patients with suspected nonalcoholic fatty liver disease. Hepatology 2006;44:874‐880. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
