

Low-dose whole-body CT using deep learning image reconstruction: image quality and lesion detection
- PMID: 33571010
- PMCID: PMC8506192
- DOI: 10.1259/bjr.20201329
Low-dose whole-body CT using deep learning image reconstruction: image quality and lesion detection
Abstract
Objectives: To evaluate image quality and lesion detection capabilities of low-dose (LD) portal venous phase whole-body computed tomography (CT) using deep learning image reconstruction (DLIR).
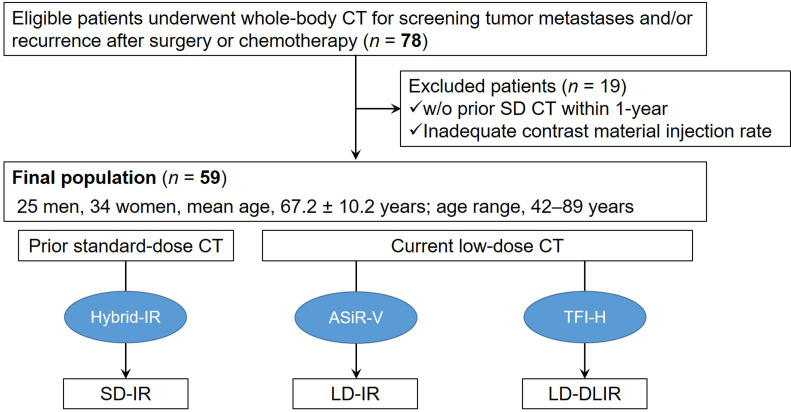
Methods: The study cohort of 59 consecutive patients (mean age, 67.2 years) who underwent whole-body LD CT and a prior standard-dose (SD) CT reconstructed with hybrid iterative reconstruction (SD-IR) within one year for surveillance of malignancy were assessed. The LD CT images were reconstructed with hybrid iterative reconstruction of 40% (LD-IR) and DLIR (LD-DLIR). The radiologists independently evaluated image quality (5-point scale) and lesion detection. Attenuation values in Hounsfield units (HU) of the liver, pancreas, spleen, abdominal aorta, and portal vein; the background noise and signal-to-noise ratio (SNR) of the liver, pancreas, and spleen were calculated. Qualitative and quantitative parameters were compared between the SD-IR, LD-IR, and LD-DLIR images. The CT dose-index volumes (CTDIvol) and dose-length product (DLP) were compared between SD and LD scans.
Results: The image quality and lesion detection rate of the LD-DLIR was comparable to the SD-IR. The image quality was significantly better in SD-IR than in LD-IR (p < 0.017). The attenuation values of all anatomical structures were comparable between the SD-IR and LD-DLIR (p = 0.28-0.96). However, background noise was significantly lower in the LD-DLIR (p < 0.001) and resulted in improved SNRs (p < 0.001) compared to the SD-IR and LD-IR images. The mean CTDIvol and DLP were significantly lower in the LD (2.9 mGy and 216.2 mGy•cm) than in the SD (13.5 mGy and 1011.6 mGy•cm) (p < 0.0001).
Conclusion: LD CT images reconstructed with DLIR enable radiation dose reduction of >75% while maintaining image quality and lesion detection rate and superior SNR in comparison to SD-IR.
Advances in knowledge: Deep learning image reconstruction algorithm enables around 80% reduction in radiation dose while maintaining the image quality and lesion detection compared to standard-dose whole-body CT.
Conflict of interest statement
Figures


Similar articles
-
Deep learning reconstruction CT for liver metastases: low-dose dual-energy vs standard-dose single-energy.Eur Radiol. 2024 Jan;34(1):28-38. doi: 10.1007/s00330-023-10033-3. Epub 2023 Aug 2. Eur Radiol. 2024. PMID: 37532899
-
Deep-learning CT reconstruction in clinical scans of the abdomen: a systematic review and meta-analysis.Abdom Radiol (NY). 2023 Aug;48(8):2724-2756. doi: 10.1007/s00261-023-03966-2. Epub 2023 Jun 6. Abdom Radiol (NY). 2023. PMID: 37280374 Free PMC article.
-
Deep learning image reconstruction for pancreatic low-dose computed tomography: comparison with hybrid iterative reconstruction.Abdom Radiol (NY). 2021 Sep;46(9):4238-4244. doi: 10.1007/s00261-021-03111-x. Epub 2021 May 11. Abdom Radiol (NY). 2021. PMID: 33973060
-
Deep learning image reconstruction for improvement of image quality of abdominal computed tomography: comparison with hybrid iterative reconstruction.Jpn J Radiol. 2021 Jun;39(6):598-604. doi: 10.1007/s11604-021-01089-6. Epub 2021 Jan 15. Jpn J Radiol. 2021. PMID: 33449305
-
Influence of deep learning image reconstruction algorithm for reducing radiation dose and image noise compared to iterative reconstruction and filtered back projection for head and chest computed tomography examinations: a systematic review.F1000Res. 2024 Apr 15;13:274. doi: 10.12688/f1000research.147345.1. eCollection 2024. F1000Res. 2024. PMID: 38725640 Free PMC article.
Cited by
-
Application of Deep Learning-Based Denoising Technique for Radiation Dose Reduction in Dynamic Abdominal CT: Comparison with Standard-Dose CT Using Hybrid Iterative Reconstruction Method.J Digit Imaging. 2023 Aug;36(4):1578-1587. doi: 10.1007/s10278-023-00808-x. Epub 2023 Mar 21. J Digit Imaging. 2023. PMID: 36944812 Free PMC article.
-
Coronary atherosclerotic plaque characterization with silicon-based photon-counting computed tomography (CT): A simulation-based feasibility study.Med Phys. 2024 Dec;51(12):8725-8741. doi: 10.1002/mp.17422. Epub 2024 Sep 25. Med Phys. 2024. PMID: 39321385
-
Deep learning reconstruction CT for liver metastases: low-dose dual-energy vs standard-dose single-energy.Eur Radiol. 2024 Jan;34(1):28-38. doi: 10.1007/s00330-023-10033-3. Epub 2023 Aug 2. Eur Radiol. 2024. PMID: 37532899
-
Deep-learning CT reconstruction in clinical scans of the abdomen: a systematic review and meta-analysis.Abdom Radiol (NY). 2023 Aug;48(8):2724-2756. doi: 10.1007/s00261-023-03966-2. Epub 2023 Jun 6. Abdom Radiol (NY). 2023. PMID: 37280374 Free PMC article.
-
Virtual Surgical Planning, 3D-Printing and Customized Bone Allograft for Acute Correction of Severe Genu Varum in Children.J Pers Med. 2022 Dec 12;12(12):2051. doi: 10.3390/jpm12122051. J Pers Med. 2022. PMID: 36556271 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
