

Quantifying asymptomatic infection and transmission of COVID-19 in New York City using observed cases, serology, and testing capacity
- PMID: 33571106
- PMCID: PMC7936345
- DOI: 10.1073/pnas.2019716118
Quantifying asymptomatic infection and transmission of COVID-19 in New York City using observed cases, serology, and testing capacity
Abstract
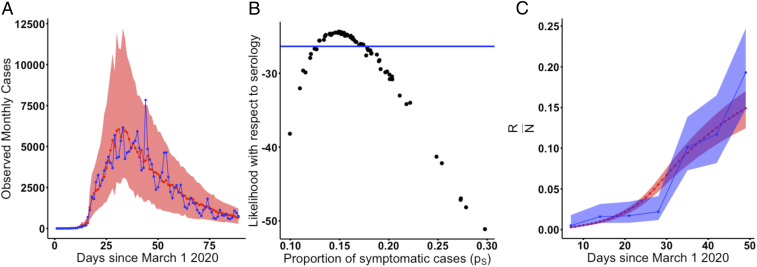
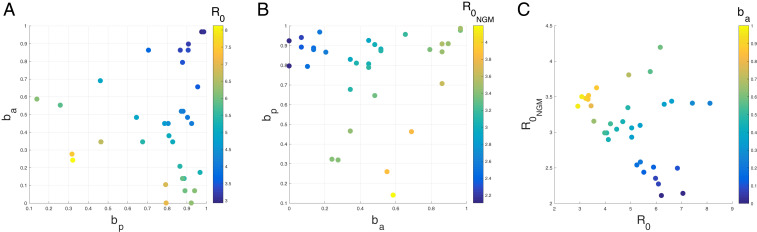
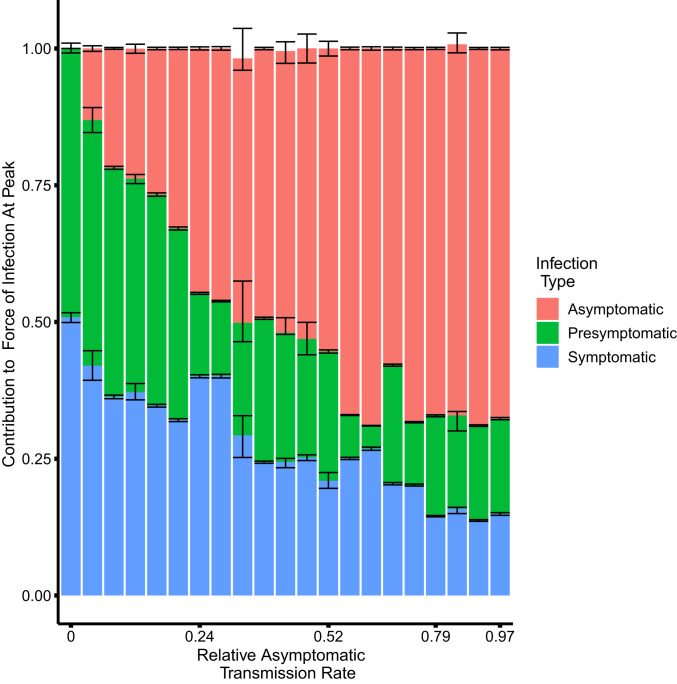
The contributions of asymptomatic infections to herd immunity and community transmission are key to the resurgence and control of COVID-19, but are difficult to estimate using current models that ignore changes in testing capacity. Using a model that incorporates daily testing information fit to the case and serology data from New York City, we show that the proportion of symptomatic cases is low, ranging from 13 to 18%, and that the reproductive number may be larger than often assumed. Asymptomatic infections contribute substantially to herd immunity, and to community transmission together with presymptomatic ones. If asymptomatic infections transmit at similar rates as symptomatic ones, the overall reproductive number across all classes is larger than often assumed, with estimates ranging from 3.2 to 4.4. If they transmit poorly, then symptomatic cases have a larger reproductive number ranging from 3.9 to 8.1. Even in this regime, presymptomatic and asymptomatic cases together comprise at least 50% of the force of infection at the outbreak peak. We find no regimes in which all infection subpopulations have reproductive numbers lower than three. These findings elucidate the uncertainty that current case and serology data cannot resolve, despite consideration of different model structures. They also emphasize how temporal data on testing can reduce and better define this uncertainty, as we move forward through longer surveillance and second epidemic waves. Complementary information is required to determine the transmissibility of asymptomatic cases, which we discuss. Regardless, current assumptions about the basic reproductive number of severe acute respiratory syndrome coronavirus 2 (SARS-Cov-2) should be reconsidered.
Keywords: COVID-19; asymptomatic transmission; epidemiological model; epidemiological parameter estimates; testing submodel.
Copyright © 2021 the Author(s). Published by PNAS.
Conflict of interest statement
The authors declare no competing interest.
Figures


References
-
- Paules C. I., Marston H. D., Fauci A. S., Coronavirus infections—More than just the common cold. JAMA 323, 707–708 (2020). - PubMed
-
- Centers for Disease Control and Prevention , Overview of testing for SARS-CoV-2 (COVID-19). https://www.cdc.gov/coronavirus/2019-ncov/hcp/testing-overview.html. Accessed 7 August 2020.
-
- Majumder M., Mandl K. D., Early transmissibility assessment of a novel coronavirus in Wuhan, China. SSRN [Preprint] (2020). 10.2139/ssrn.3524675 (Accessed January 26, 2020). - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
