

Durable SARS-CoV-2 B cell immunity after mild or severe disease
- PMID: 33571162
- PMCID: PMC8011891
- DOI: 10.1172/JCI145516
Durable SARS-CoV-2 B cell immunity after mild or severe disease
Abstract
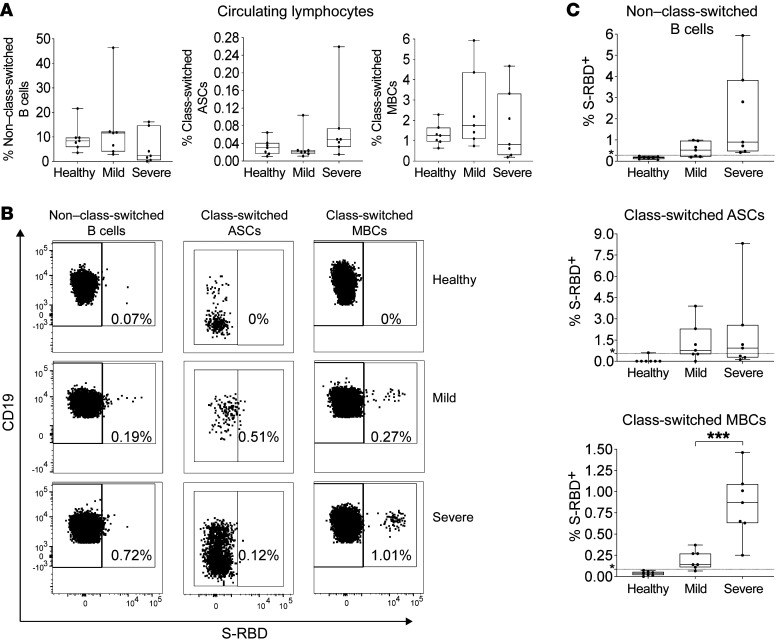
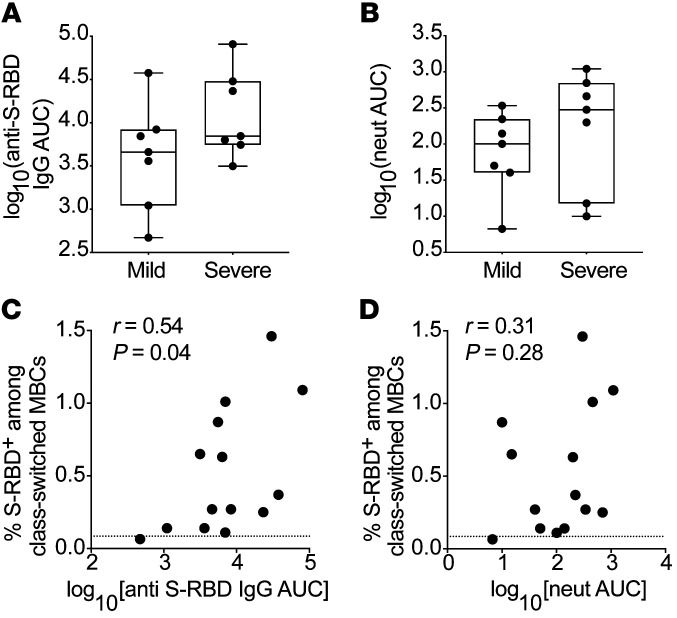
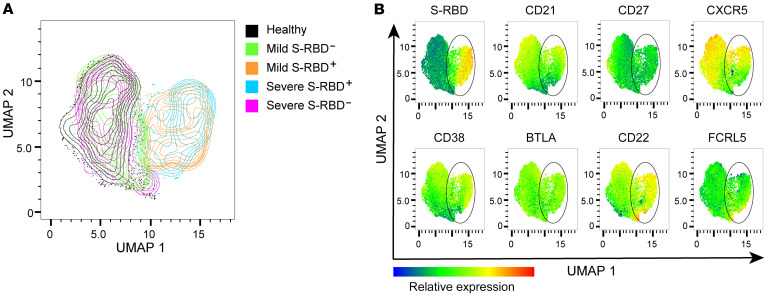
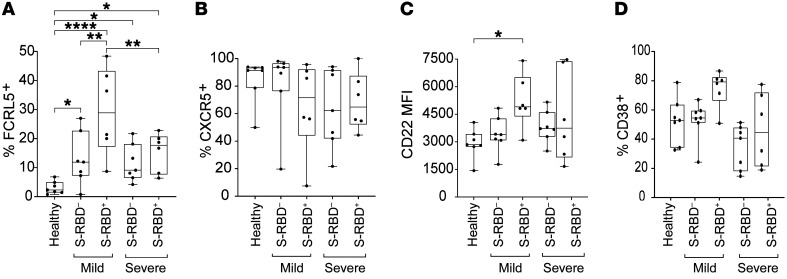
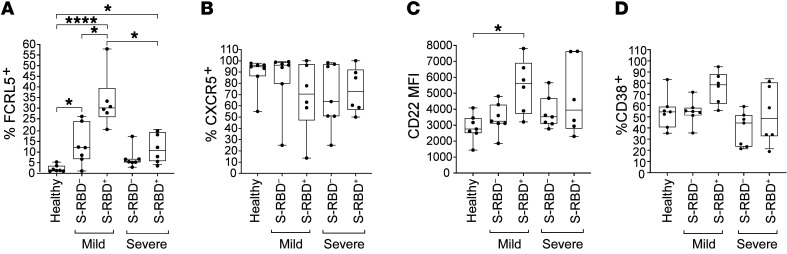
Multiple studies have shown loss of severe acute respiratory syndrome coronavirus 2-specific (SARS-CoV-2-specific) antibodies over time after infection, raising concern that humoral immunity against the virus is not durable. If immunity wanes quickly, millions of people may be at risk for reinfection after recovery from coronavirus disease 2019 (COVID-19). However, memory B cells (MBCs) could provide durable humoral immunity even if serum neutralizing antibody titers decline. We performed multidimensional flow cytometric analysis of S protein receptor binding domain-specific (S-RBD-specific) MBCs in cohorts of ambulatory patients with COVID-19 with mild disease (n = 7), and hospitalized patients with moderate to severe disease (n = 7), at a median of 54 days (range, 39-104 days) after symptom onset. We detected S-RBD-specific class-switched MBCs in 13 of 14 participants, failing only in the individual with the lowest plasma levels of anti-S-RBD IgG and neutralizing antibodies. Resting MBCs (rMBCs) made up the largest proportion of S-RBD-specific MBCs in both cohorts. FCRL5, a marker of functional memory on rMBCs, was more dramatically upregulated on S-RBD-specific rMBCs after mild infection than after severe infection. These data indicate that most SARS-CoV-2-infected individuals develop S-RBD-specific, class-switched rMBCs that resemble germinal center-derived B cells induced by effective vaccination against other pathogens, providing evidence for durable B cell-mediated immunity against SARS-CoV-2 after mild or severe disease.
Keywords: Adaptive immunity; Beta cells; Immunology; Infectious disease.
Conflict of interest statement
Figures

Update of
-
Durable SARS-CoV-2 B cell immunity after mild or severe disease.medRxiv [Preprint]. 2020 Oct 30:2020.10.28.20220996. doi: 10.1101/2020.10.28.20220996. medRxiv. 2020. Update in: J Clin Invest. 2021 Apr 1;131(7):145516. doi: 10.1172/JCI145516. PMID: 33140070 Free PMC article. Updated. Preprint.
References
-
- Guan WJ, Zhong NS. Clinical characteristics of Covid-19 in China. Reply. N Engl J Med. 2020;382(19):1861–1862. - PubMed
-
- doi: 10.1101/2020.07.09.20148429. Seow J, et al. Longitudinal evaluation and decline of antibody responses in SARS-CoV-2 infection [preprint]. Posted on medRxiv July 11, 2020. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
