

The role of children in the spread of COVID-19: Using household data from Bnei Brak, Israel, to estimate the relative susceptibility and infectivity of children
- PMID: 33571188
- PMCID: PMC7877572
- DOI: 10.1371/journal.pcbi.1008559
The role of children in the spread of COVID-19: Using household data from Bnei Brak, Israel, to estimate the relative susceptibility and infectivity of children
Abstract
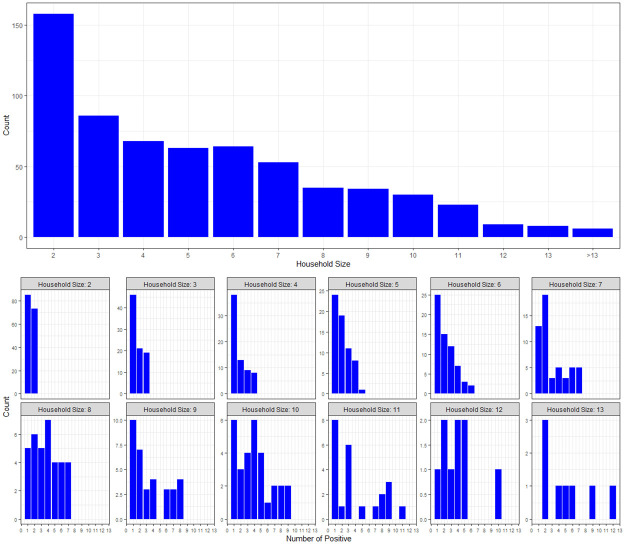
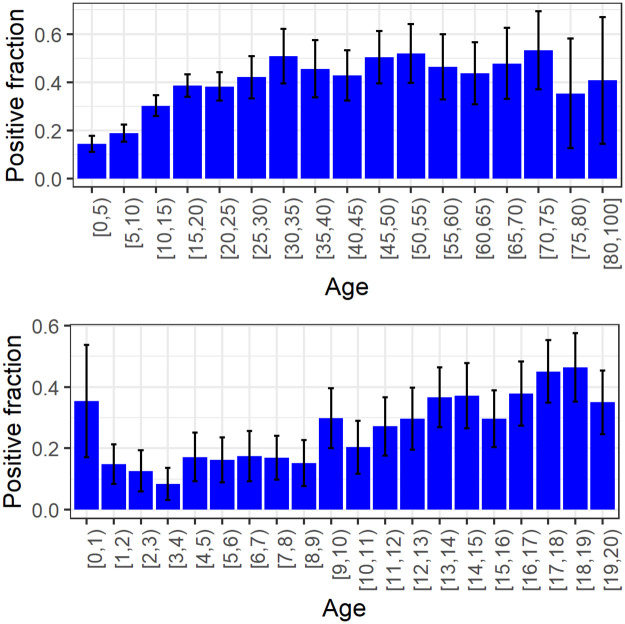
One of the significant unanswered questions about COVID-19 epidemiology relates to the role of children in transmission. This study uses data on infections within households in order to estimate the susceptibility and infectivity of children compared to those of adults. The data were collected from households in the city of Bnei Brak, Israel, in which all household members were tested for COVID-19 using PCR (637 households, average household size of 5.3). In addition, serological tests were performed on a subset of the individuals in the study. Inspection of the PCR data shows that children are less likely to be tested positive compared to adults (25% of children positive over all households, 44% of adults positive over all households, excluding index cases), and the chance of being positive increases with age. Analysis of joint PCR/serological data shows that there is under-detection of infections in the PCR testing, which is more substantial in children. However, the differences in detection rates are not sufficient to account for the differences in PCR positive rates in the two age groups. To estimate relative transmission parameters, we employ a discrete stochastic model of the spread of infection within a household, allowing for susceptibility and infectivity parameters to differ among children and adults. The model is fitted to the household data using a simulated maximum likelihood approach. To adjust parameter estimates for under-detection of infections in the PCR results, we employ a multiple imputation procedure using estimates of under-detection in children and adults, based on the available serological data. We estimate that the susceptibility of children (under 20 years old) is 43% (95% CI: [31%, 55%]) of the susceptibility of adults. The infectivity of children was estimated to be 63% (95% CI: [37%, 88%]) relative to that of adults.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, et al. Epidemiology of COVID-19 Among Children in China. Pediatrics. 2020;145(6). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
