

Virus Etiology, Diversity and Clinical Characteristics in South African Children Hospitalised with Gastroenteritis
- PMID: 33573340
- PMCID: PMC7911269
- DOI: 10.3390/v13020215
Virus Etiology, Diversity and Clinical Characteristics in South African Children Hospitalised with Gastroenteritis
Abstract
Background: Viral gastroenteritis remains a major cause of hospitalisation in young children. This study aimed to determine the distribution and diversity of enteric viruses in children ≤5 years, hospitalised with gastroenteritis at Kalafong Provincial Tertiary Hospital, Pretoria, South Africa, between July 2016 and December 2017.
Methods: Stool specimens (n = 205) were screened for norovirus GI and GII, rotavirus, sapovirus, astrovirus and adenovirus by multiplex RT-PCR. HIV exposure and FUT2 secretor status were evaluated. Secretor status was determined by FUT2 genotyping.
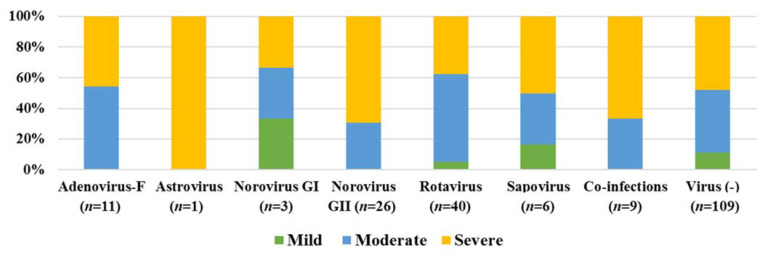
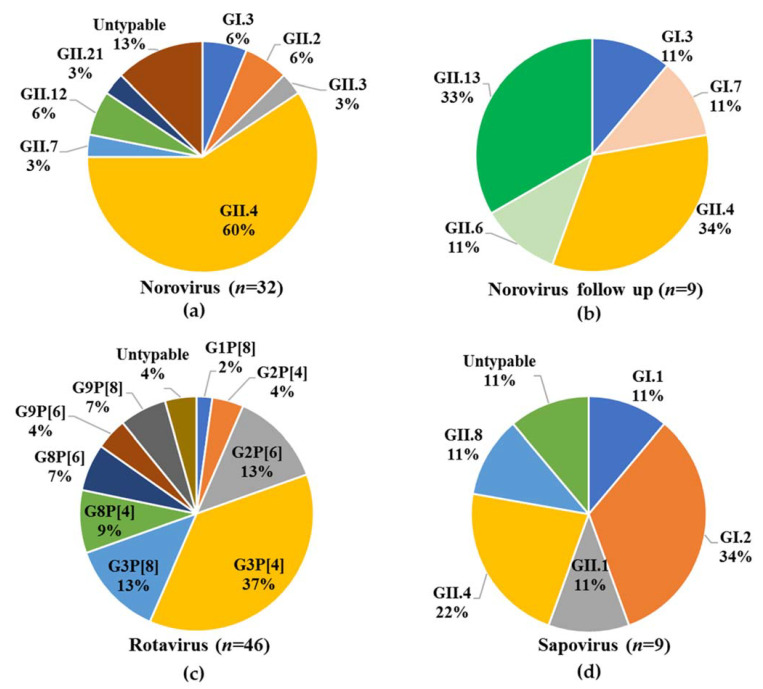
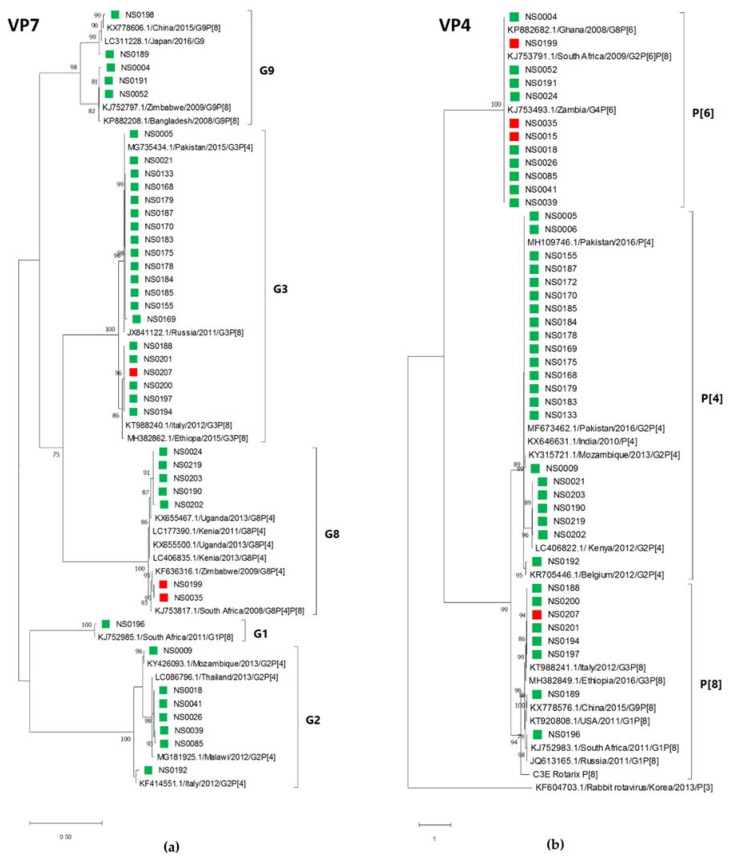
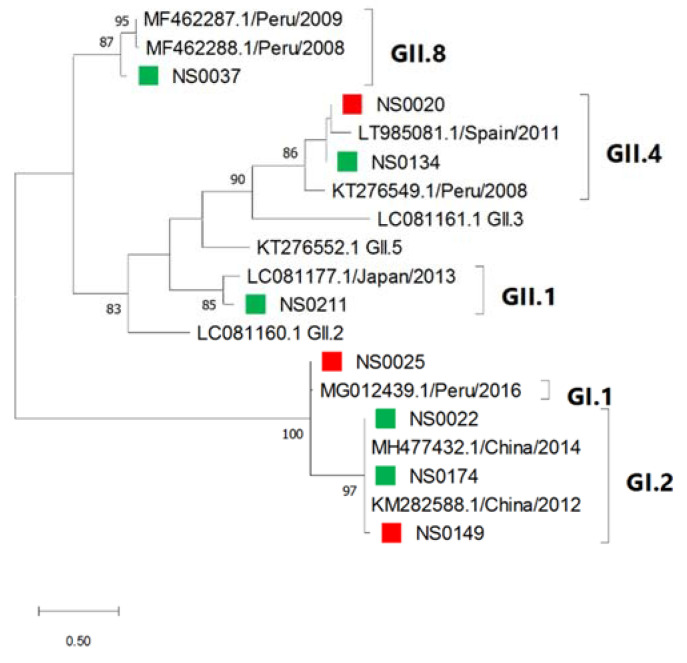
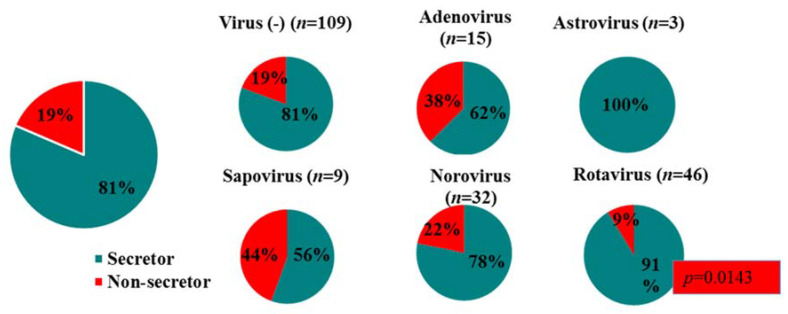
Results: At least one gastroenteritis virus was detected in 47% (96/205) of children. Rotavirus predominated (46/205), followed by norovirus (32/205), adenovirus (15/205), sapovirus (9/205) and astrovirus (3/205). Norovirus genotypes GI.3, GII.2, GII.3, GII.4, GII.7, GII.12, GII.21, and rotavirus strains G1P[8], G2P[4], G2P[6], G3P[4], G3P[8], G8P[4], G8P[6], G9P[6], G9P[8] and sapovirus genotypes GI.1, GI.2, GII.1, GII.4, GII.8 were detected; norovirus GII.4[P31] and rotavirus G3P[4] predominated. Asymptomatic norovirus infection (GI.3, GI.7, GII.4, GII.6, GII.13) was detected in 22% of 46 six-week follow up stools. HIV exposure (30%) was not associated with more frequent or severe viral gastroenteritis hospitalisations compared to unexposed children. Rotavirus preferentially infected secretor children (p = 0.143) and norovirus infected 78% secretors and 22% non-secretors.
Conclusion: Rotavirus was still the leading cause of gastroenteritis hospitalisations, but norovirus caused more severe symptoms.
Keywords: FUT2 secretor status; HIV exposure; norovirus; paediatric gastroenteritis; rotavirus.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures



References
-
- Institute for Health Metrics and Evaluation (IHME) Findings from the Global Burden of Disease Study 2017. IHME; Seattle, WA, USA: 2018.
-
- Troeger C., Khalil I.A., Rao P.C., Cao S., Blacker B.F., Ahmed T., Armah G., Bines J.E., Brewer T.G., Colombara D.V. Rotavirus vaccination and the global burden of rotavirus diarrhea among children younger than 5 years. JAMA Pediatr. 2018;172:958–965. doi: 10.1001/jamapediatrics.2018.1960. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
