

Clinical, radiographical and histological evaluation of alveolar ridge preservation with an autogenous tooth derived particulate graft in EDS class 3-4 defects
- PMID: 33573644
- PMCID: PMC7879529
- DOI: 10.1186/s12903-021-01429-y
Clinical, radiographical and histological evaluation of alveolar ridge preservation with an autogenous tooth derived particulate graft in EDS class 3-4 defects
Abstract
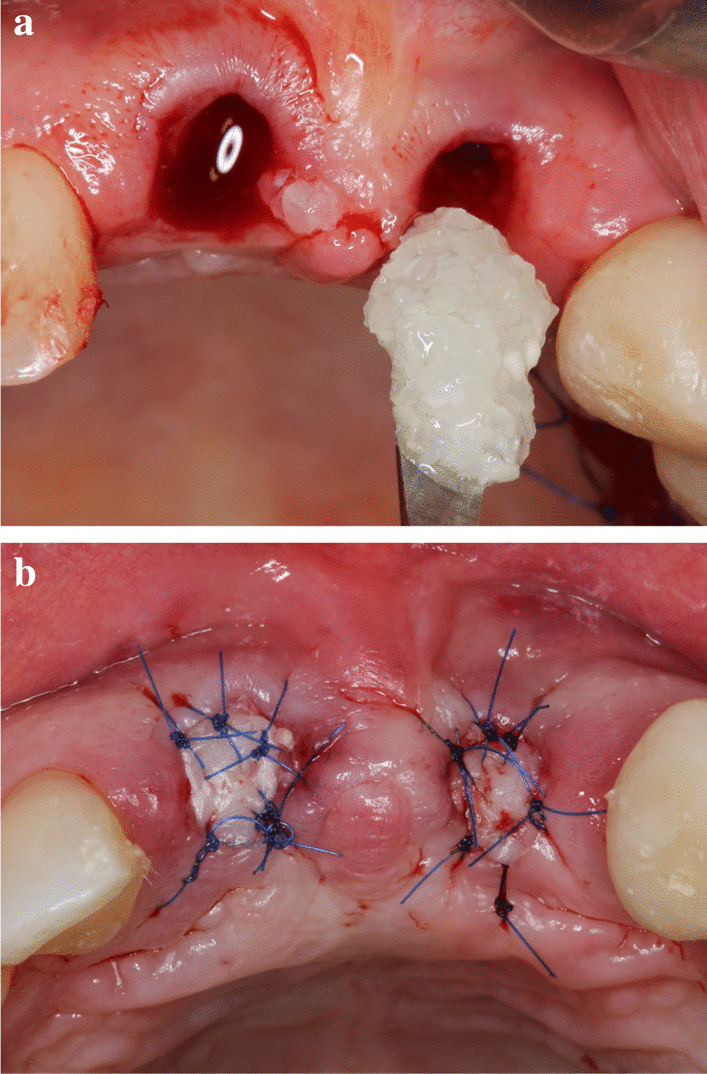
Background: The shrinkage of alveolar bone dimensions after tooth extraction is a well-known issue. This clinical phenomenon poses a challenge for clinicians aiming at implant-prosthetic treatment. BonMaker® ATB is a novel autogenous bone grafting material, produced by the mechanical and chemical processing of natural teeth. This pilot case report aims at providing a clinical, radiographical, and histological evaluation of the safety and efficacy of Bonmaker ATB powder in the treatment of EDS class 3-4 postextraction sockets with alveolar ridge preservation.
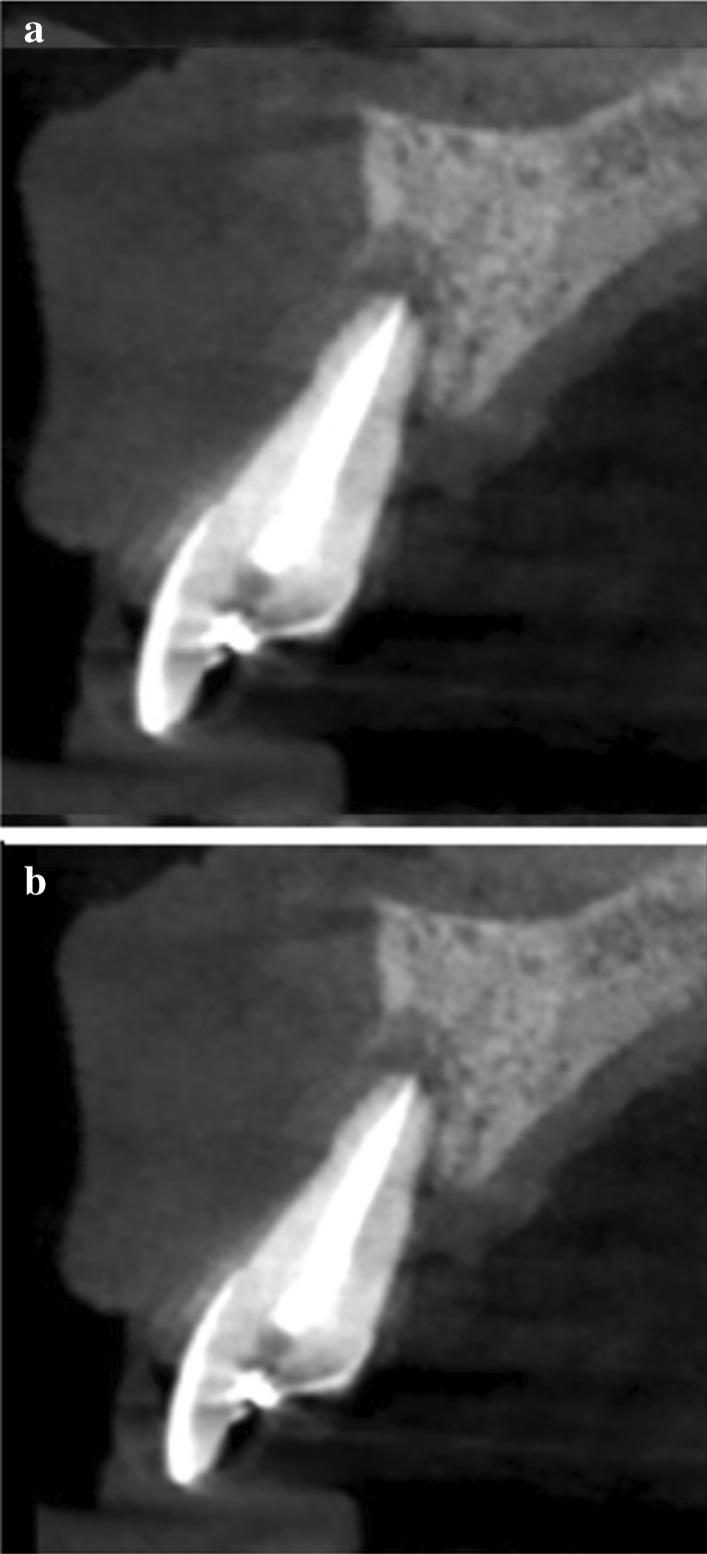
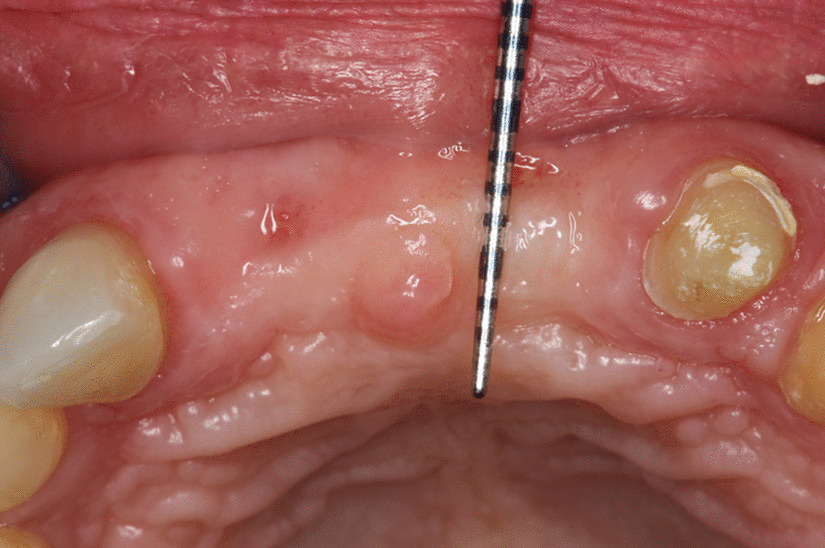
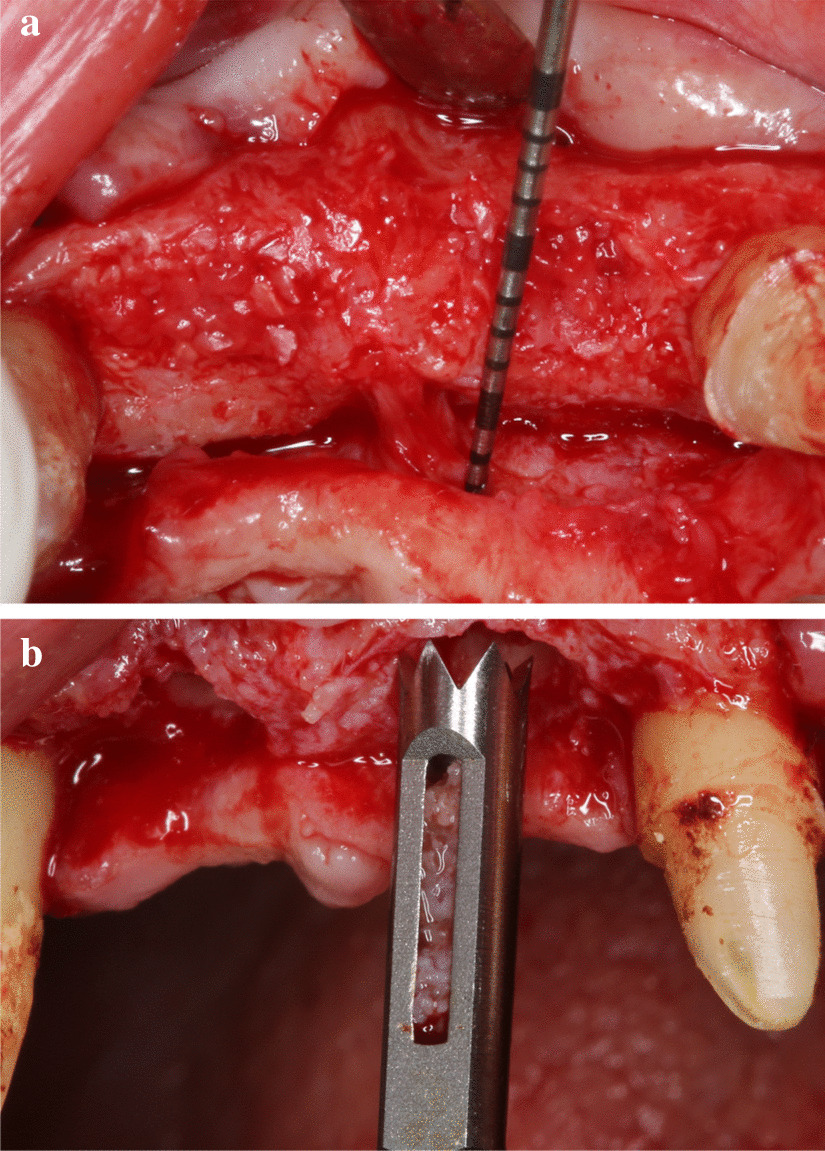
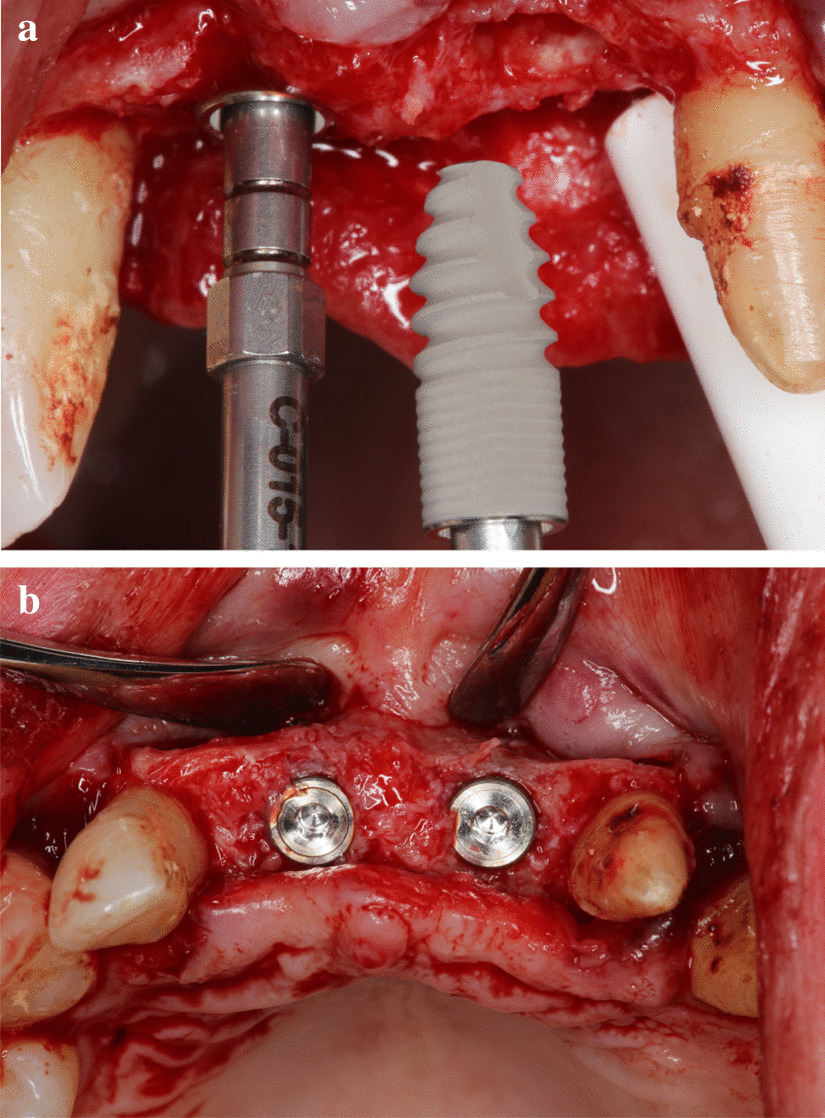
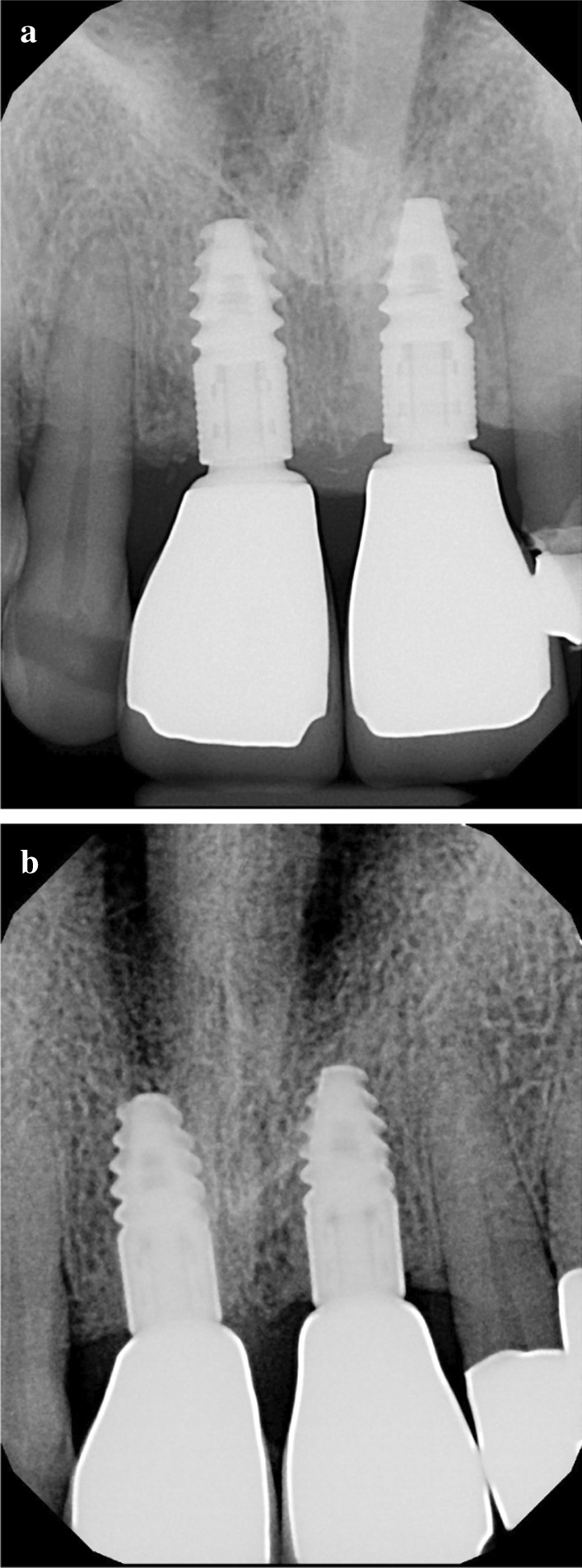
Methods: A total of 9 teeth were extracted from 5 patients. The extracted teeth were prepared immediately with the Bonmaker® device. The extraction sockets were filled up with ATB powder. Six months after extraction, standardized intraoral x-rays and CBCT scans were performed. Re-entry was performed under local anaesthesia. Core biopsies were harvested for histological analysis and implants were placed.
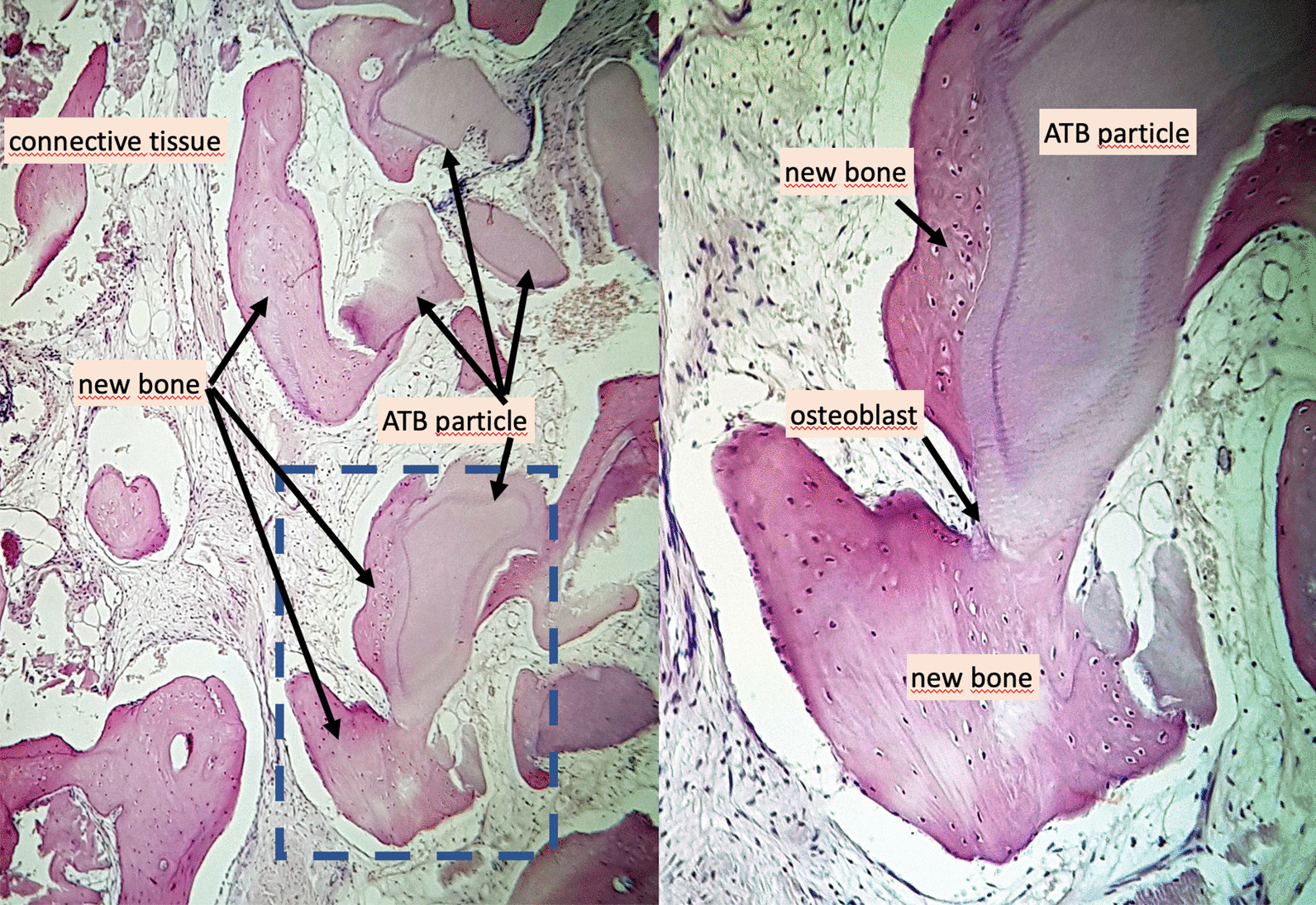
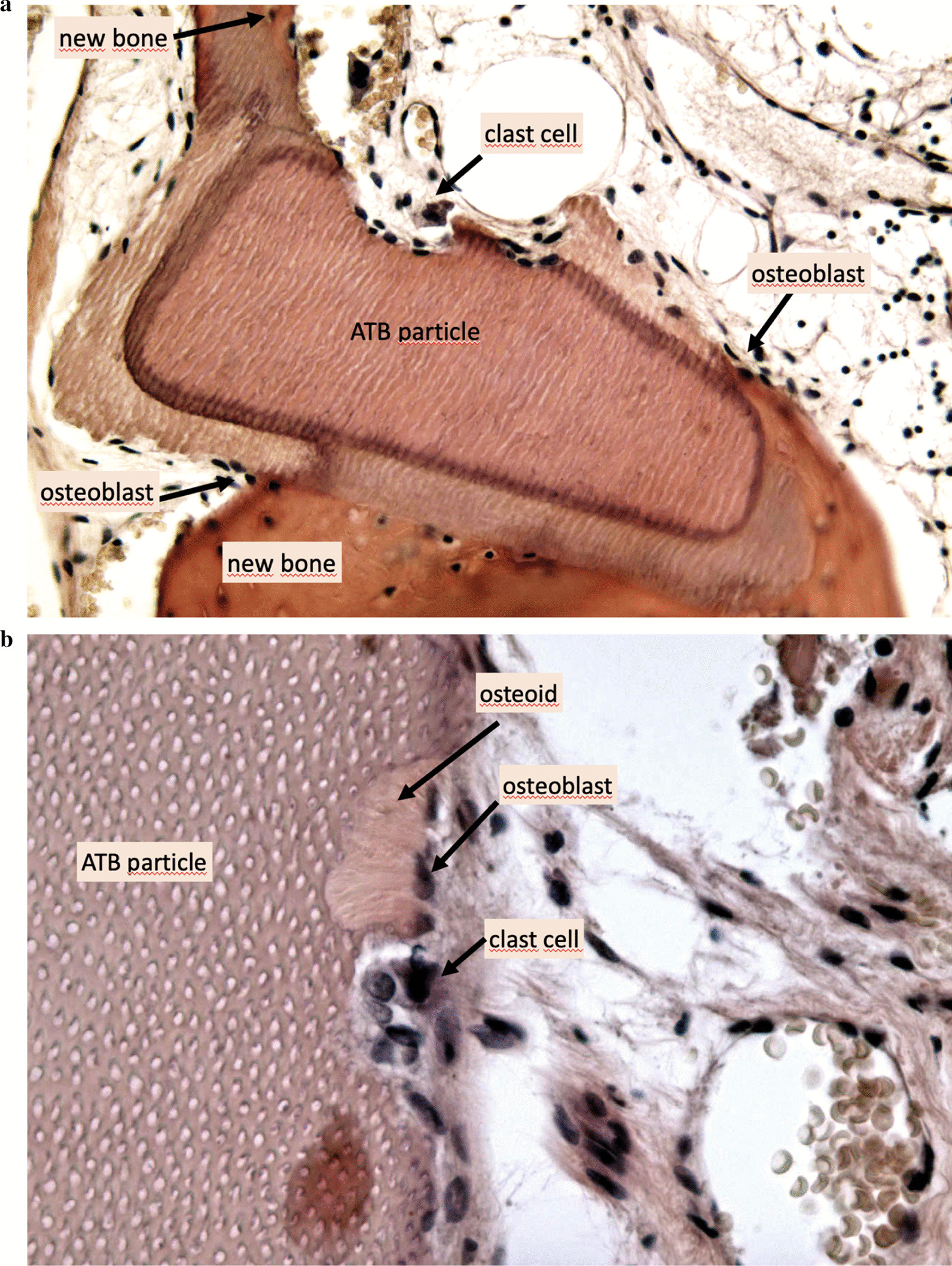
Results: Horizontal alveolar dimension loss occurred, even though ARP was performed, but the horizontal shrinkage was moderate. Vertical dimensions did not show loss of volume, but increased defect fill. Core biopsies showed ATB particles surrounded by newly formed bone and connective tissue. According to histomorphometric analysis, the harvested samples contained 56% of newly formed bone on average, and only a mean of 7% of non-remodelled ATB material was observed.
Conclusion: The preliminary clinical, radiographical, and histological results of Bonmaker® autogenous tooth graft therapy indicate that ATB may be safely and successfully used as a grafting material for ARP. Optimal graft incorporation and histologically proven effective remodelling, as well as uneventful wound healing support the clinical application of ATB to minimize post-extraction hard tissue loss. Further research is needed to exploit the full potential of ATB and to evaluate the long-term peri-implant hard and soft tissue stability of ATB-treated post-extraction sites.
Conflict of interest statement
The authors declare that they do not have other competing interests besides the funding mentioned in the Funding section.
Figures



Similar articles
-
The use of autogenous tooth bone graft is an efficient method of alveolar ridge preservation - meta-analysis and systematic review.BMC Oral Health. 2023 Apr 19;23(1):226. doi: 10.1186/s12903-023-02930-2. BMC Oral Health. 2023. PMID: 37076844 Free PMC article.
-
Efficacy of Autogenous Dentin Biomaterial on Alveolar Ridge Preservation: A Randomized Controlled Clinical Trial.Biomed Res Int. 2023 Dec 27;2023:7932432. doi: 10.1155/2023/7932432. eCollection 2023. Biomed Res Int. 2023. PMID: 38179035 Free PMC article. Clinical Trial.
-
Alveolar Ridge Preservation in the Esthetic Maxillary Zone: Tuberosity Punch Technique of Gingiva and Bone: A Pilot Study.J Contemp Dent Pract. 2021 Mar 1;22(3):290-297. J Contemp Dent Pract. 2021. PMID: 34210931
-
Evaluation of poly lactic-co-glycolic acid-coated β-tricalcium phosphate for alveolar ridge preservation: A multicenter randomized controlled trial.J Periodontol. 2021 Apr;92(4):524-535. doi: 10.1002/JPER.20-0360. Epub 2020 Oct 12. J Periodontol. 2021. PMID: 32996128 Clinical Trial.
-
Effect of alveolar ridge preservation interventions following tooth extraction: A systematic review and meta-analysis.J Clin Periodontol. 2019 Jun;46 Suppl 21:195-223. doi: 10.1111/jcpe.13057. J Clin Periodontol. 2019. PMID: 30623987
Cited by
-
Comparative Histological Analysis of Dentine-Derived Tooth Grafts in Maxillary vs Mandibular Socket Preservation: A Retrospective Study of 178 Cases.Dent J (Basel). 2024 Oct 7;12(10):320. doi: 10.3390/dj12100320. Dent J (Basel). 2024. PMID: 39452448 Free PMC article.
-
The use of autogenous tooth bone graft is an efficient method of alveolar ridge preservation - meta-analysis and systematic review.BMC Oral Health. 2023 Apr 19;23(1):226. doi: 10.1186/s12903-023-02930-2. BMC Oral Health. 2023. PMID: 37076844 Free PMC article.
-
Autogenous Tooth Bone Grafts for Repair and Regeneration of Maxillofacial Defects: A Narrative Review.Int J Environ Res Public Health. 2022 Mar 20;19(6):3690. doi: 10.3390/ijerph19063690. Int J Environ Res Public Health. 2022. PMID: 35329377 Free PMC article. Review.
-
The use of autogenous tooth bone graft powder in the treatment of osseous defects after impacted mandibular third molar extraction: a prospective split-mouth clinical pilot study.BMC Oral Health. 2022 Oct 2;22(1):433. doi: 10.1186/s12903-022-02473-y. BMC Oral Health. 2022. PMID: 36184595 Free PMC article.
-
Long-Term Results of Autologous Tooth Bone Grafting in Alveolar Cleft Reconstruction: A Retrospective Cohort Study.Biomedicines. 2025 Jul 16;13(7):1735. doi: 10.3390/biomedicines13071735. Biomedicines. 2025. PMID: 40722805 Free PMC article.
References
-
- Botticelli D, Berghlund T, Lindhe J. Hard-tissue alterations following immediate implant placement in extraction sites. J ClinPeriodontol. 2004;31(10):820–828. - PubMed
-
- Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003;23(4):313–323. - PubMed
-
- Araujo MG, Lindhe J. (2005) Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J ClinPeriodontol. 2005;32:212–218. - PubMed
-
- Van der Weiden F, Dell’Acqua F, Dagmar ES. Alveolar bone dimensional changes of post-extraction sockets in humans: a systematic review. J ClinPeriodontol. 2009;36(12):1048–1058. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
