

Natriuretic Equation to Predict Loop Diuretic Response in Patients With Heart Failure
- PMID: 33573739
- PMCID: PMC8114781
- DOI: 10.1016/j.jacc.2020.12.022
Natriuretic Equation to Predict Loop Diuretic Response in Patients With Heart Failure
Abstract
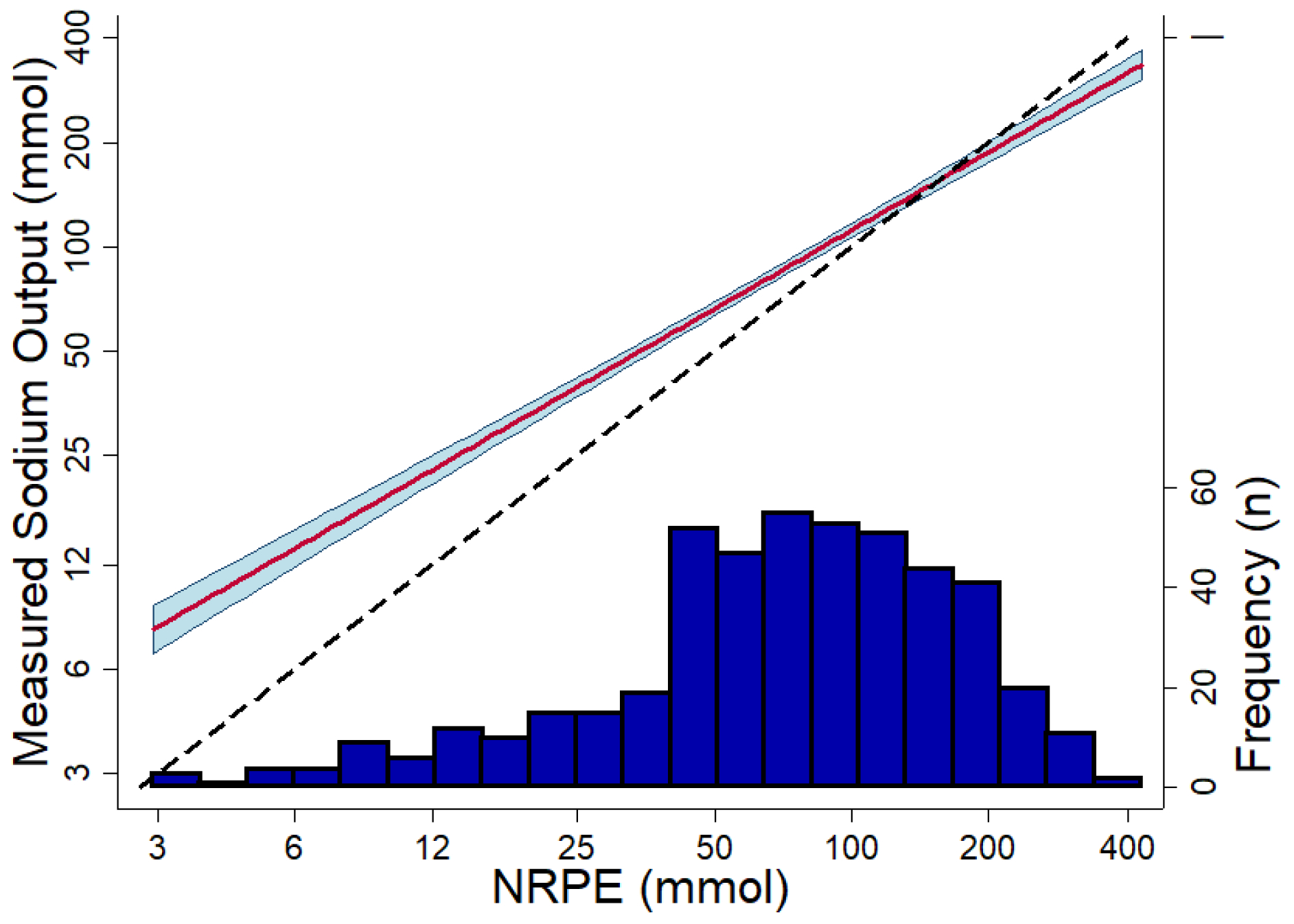
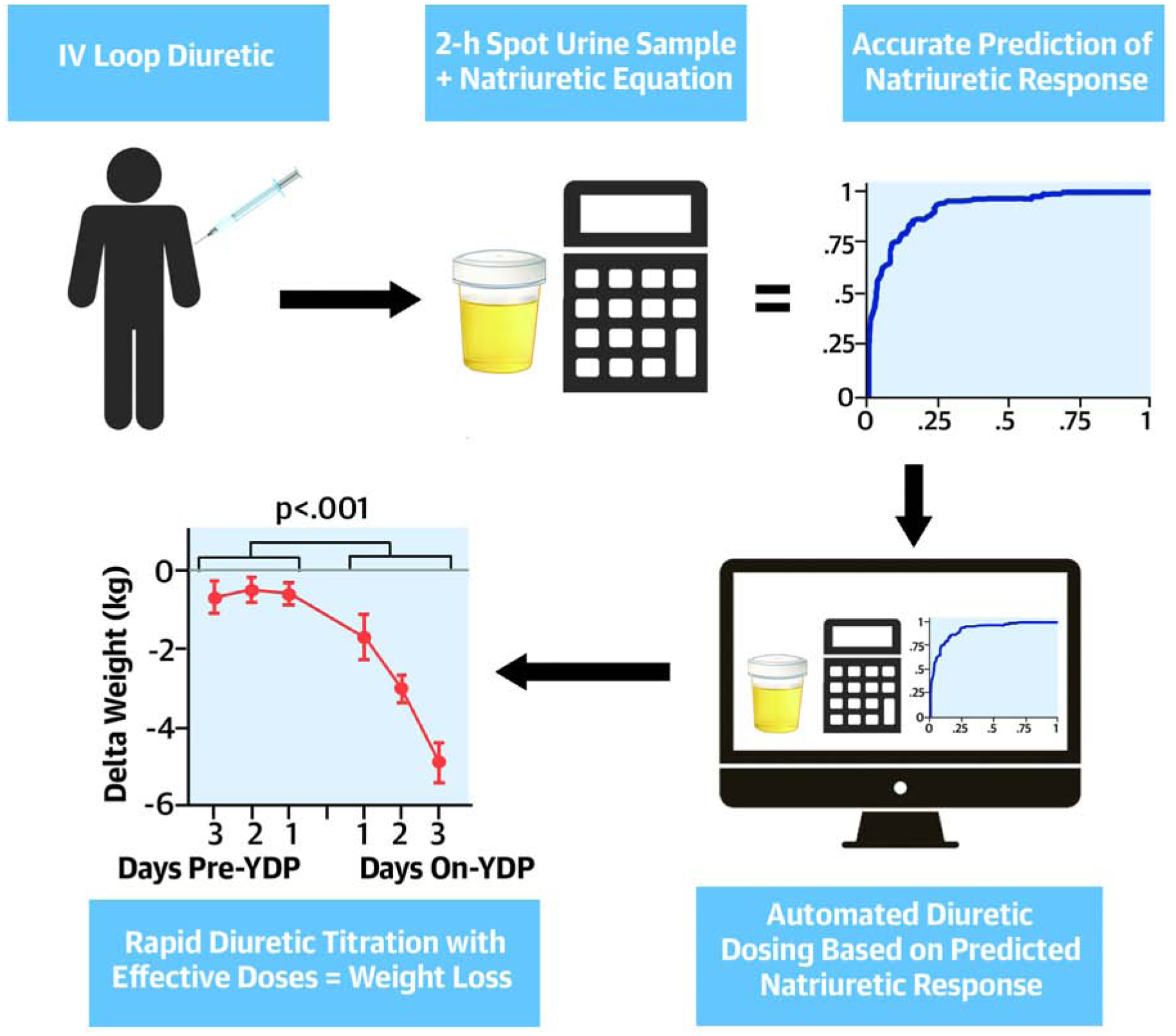
Background: Most acute decompensated heart failure admissions are driven by congestion. However, residual congestion is common and often driven by the lack of reliable tools to titrate diuretic therapy. The authors previously developed a natriuretic response prediction equation (NRPE), which predicts sodium output using a spot urine sample collected 2 h after loop diuretic administration.
Objectives: The purpose of this study was to validate the NRPE and describe proof-of-concept that the NRPE can be used to guide diuretic therapy.
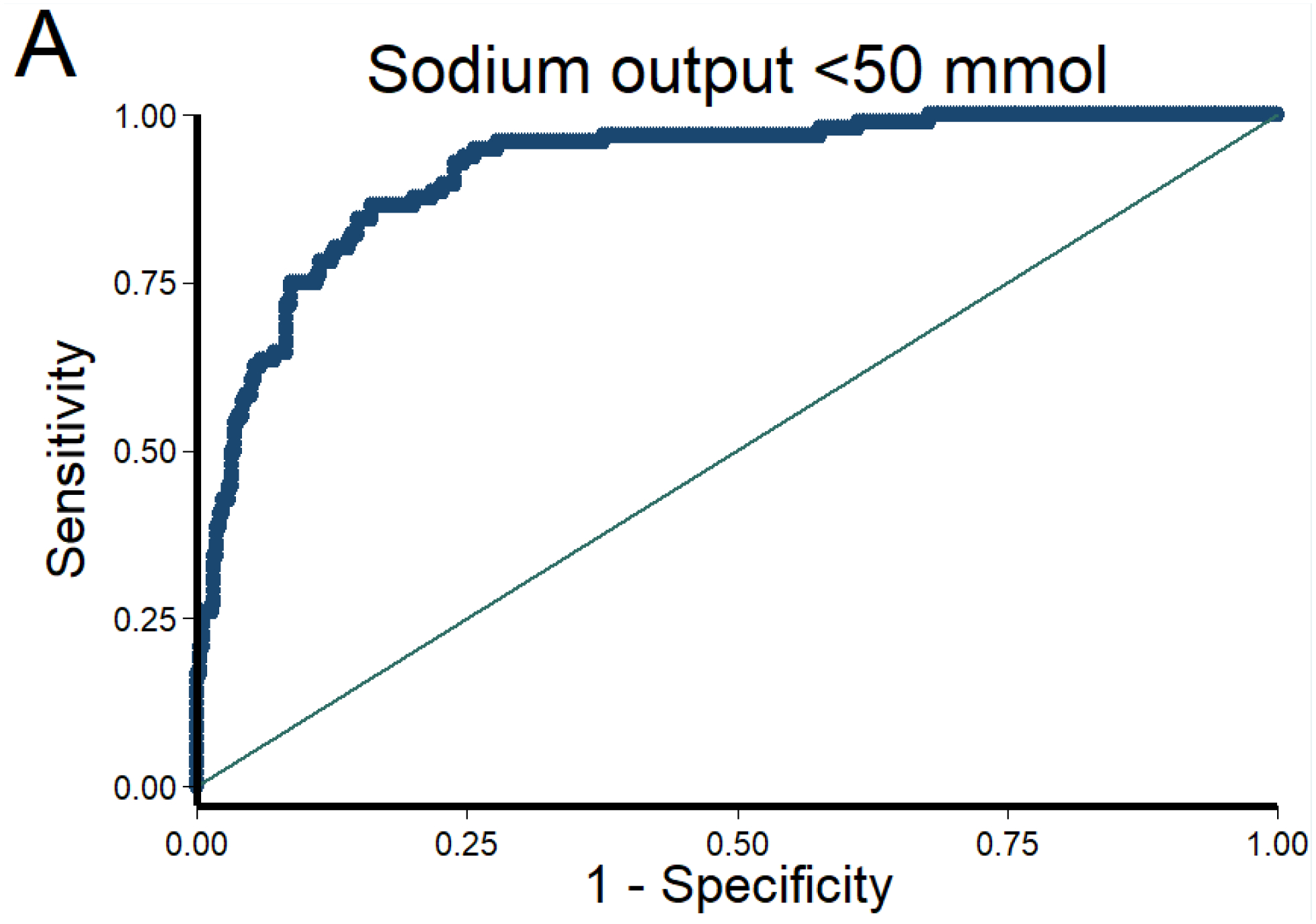
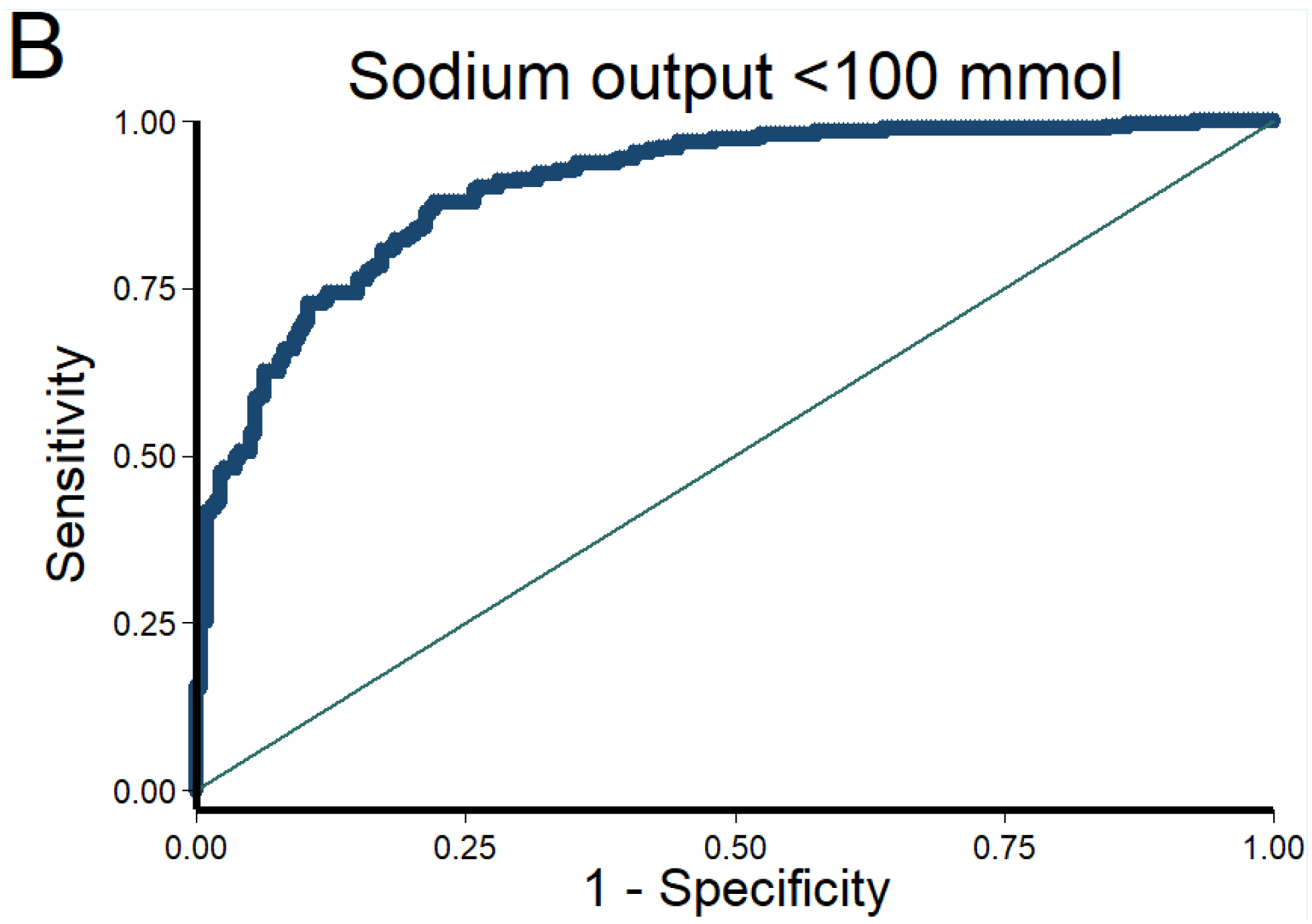
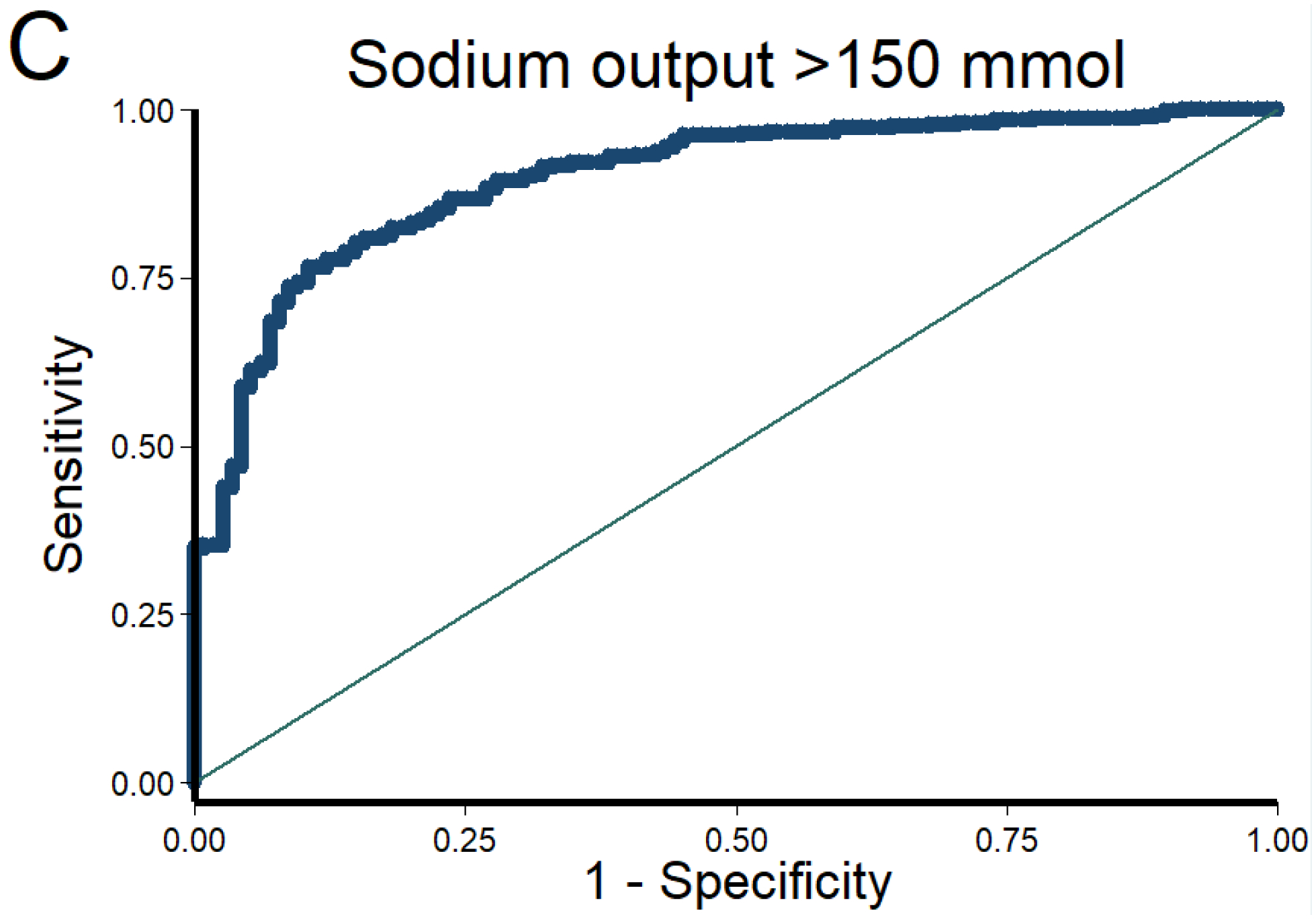
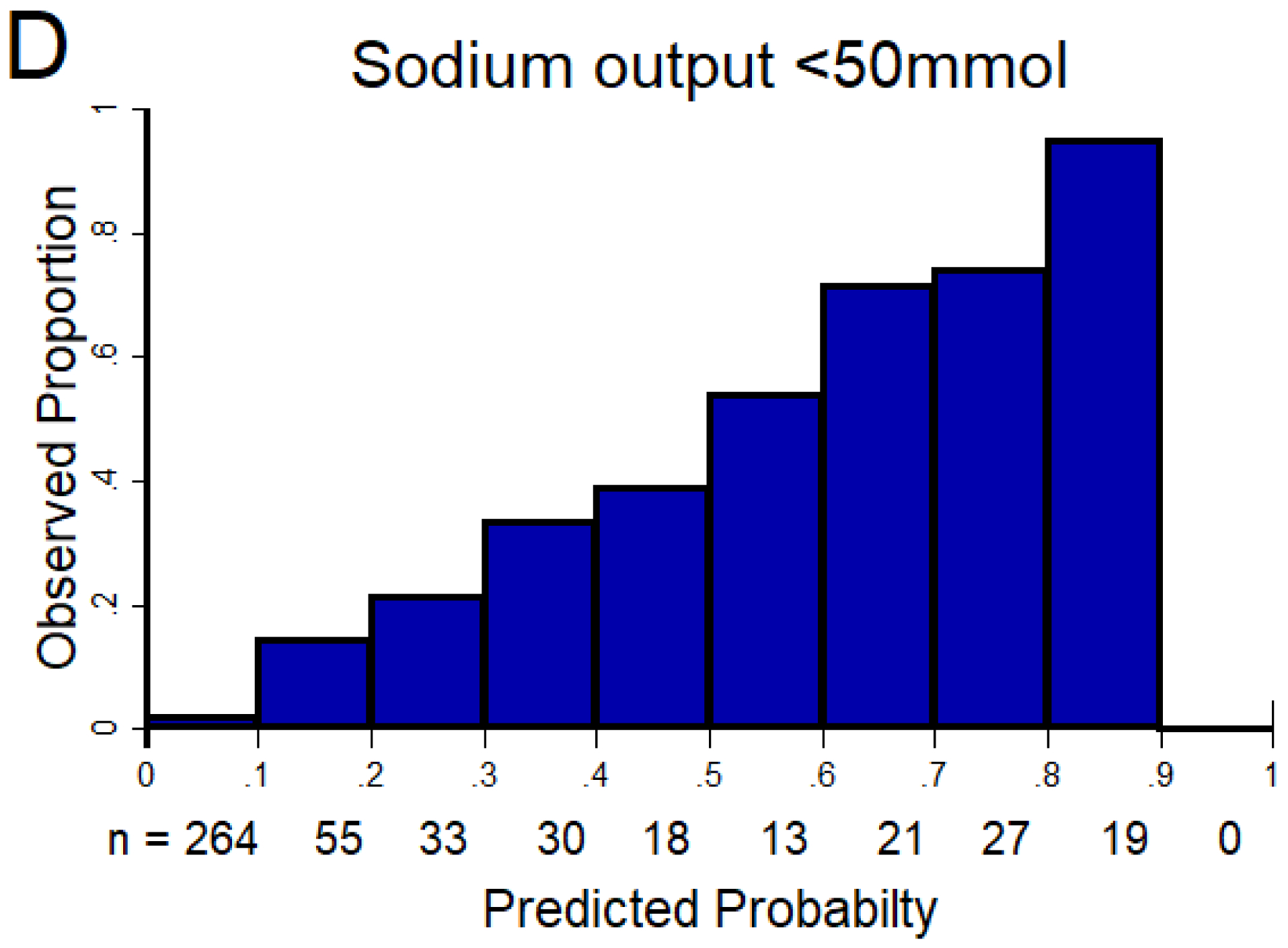
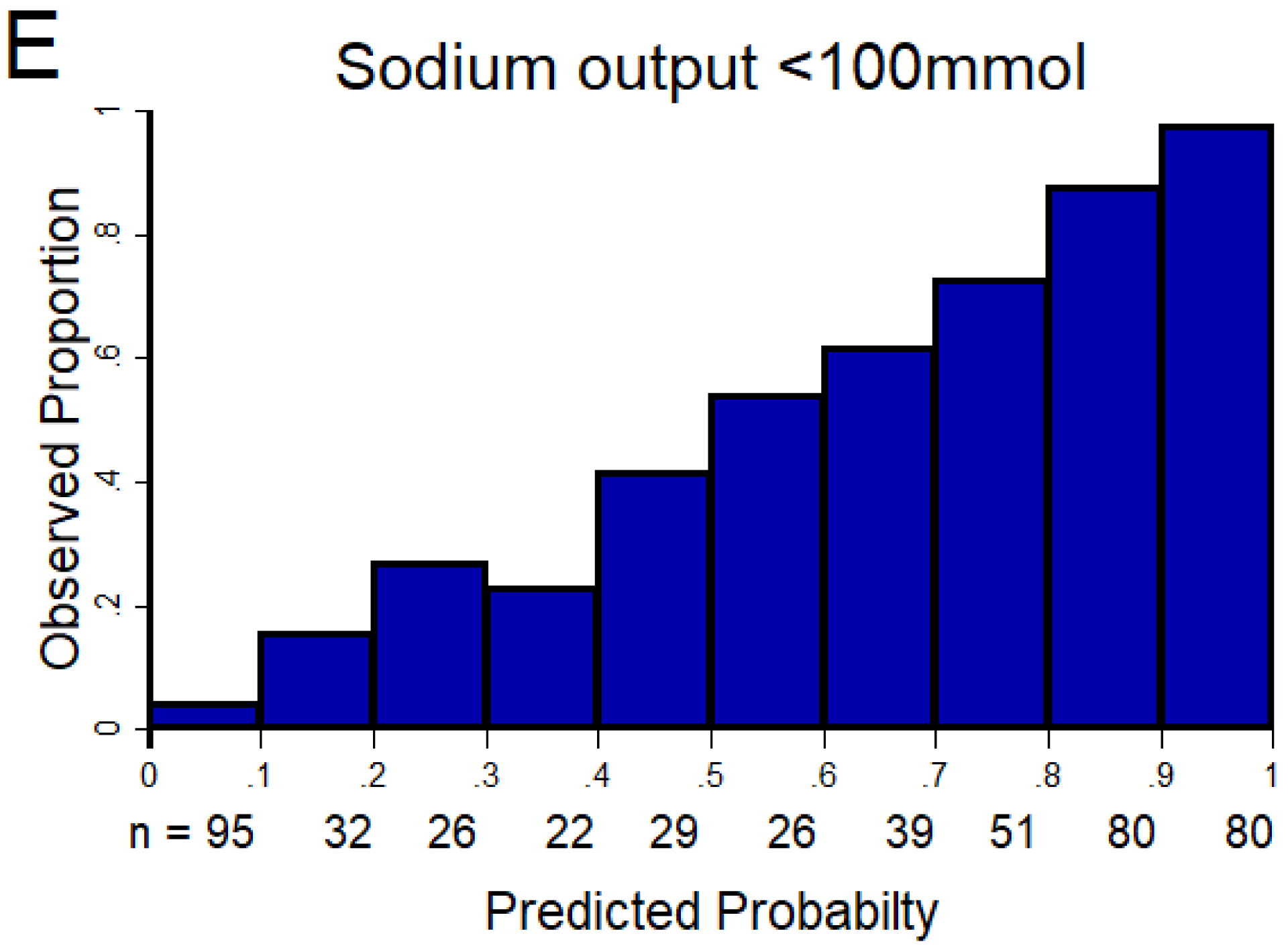
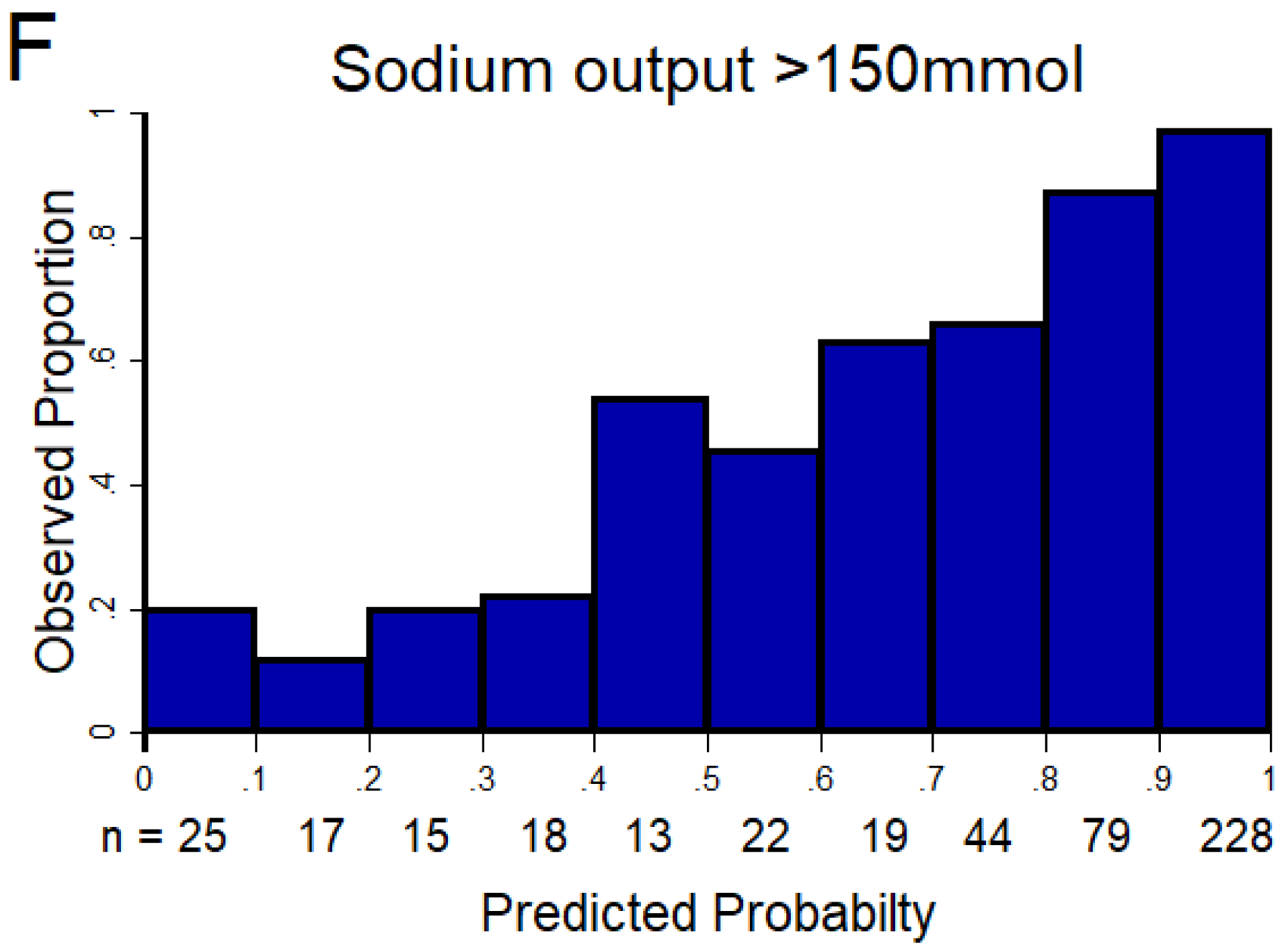
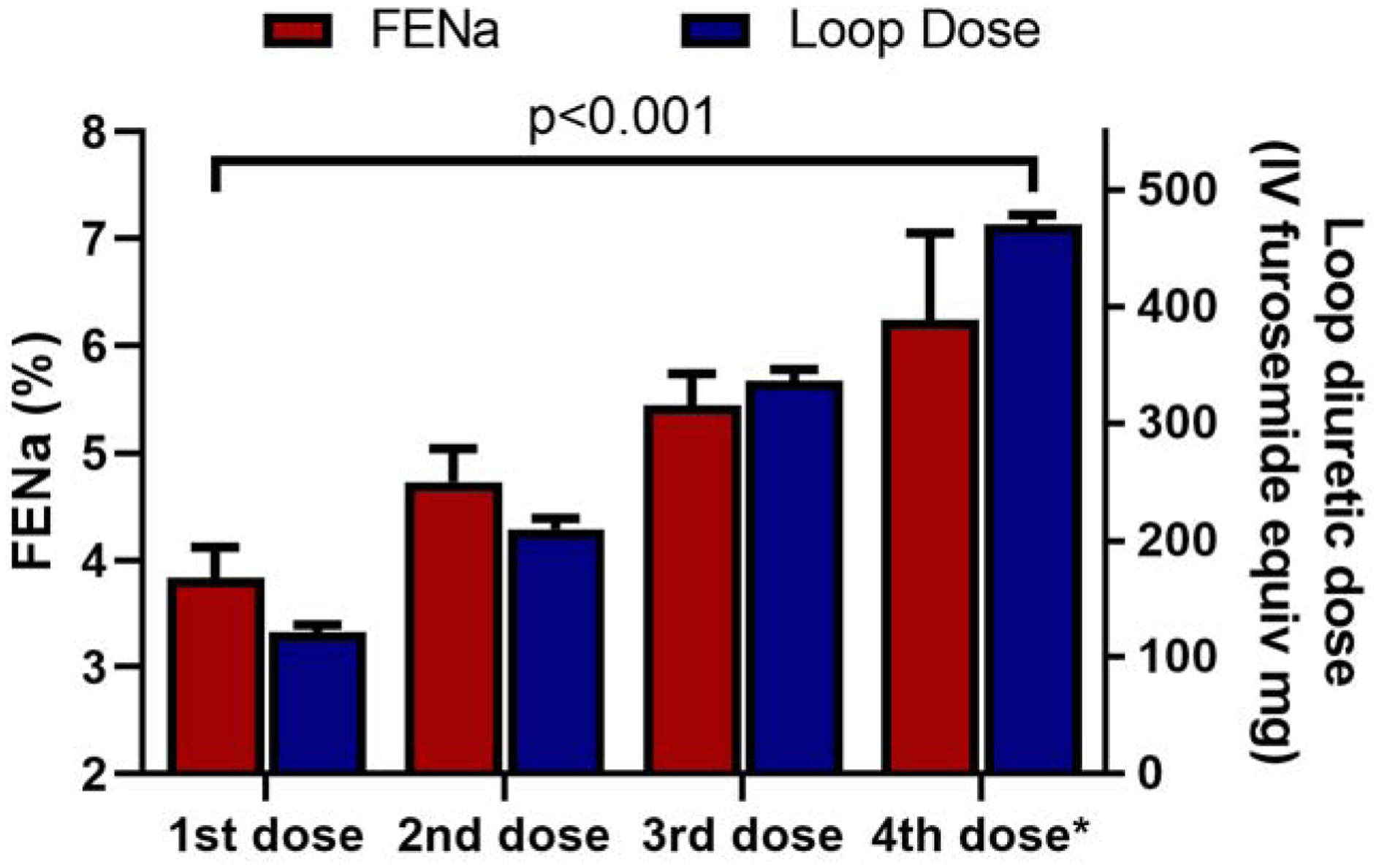
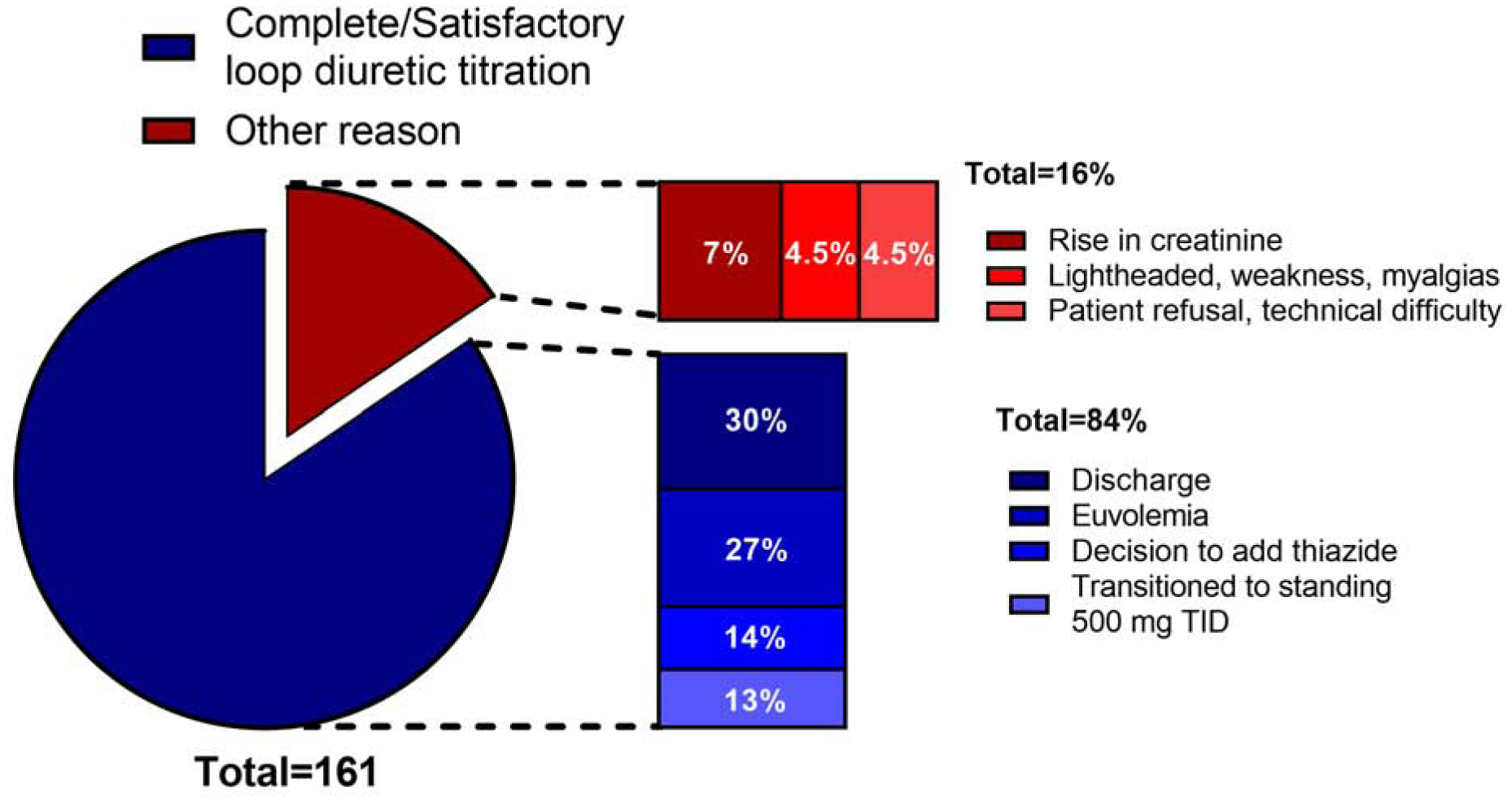
Methods: Two cohorts were assembled: 1) the Diagnosing and Targeting Mechanisms of Diuretic Resistance (MDR) cohort was used to validate the NRPE to predict 6-h sodium output after a loop diuretic, which was defined as poor (<50 mmol), suboptimal (<100 mmol), or excellent (>150 mmol); and 2) the Yale Diuretic Pathway (YDP) cohort, which used the NRPE to guide loop diuretic titration via a nurse-driven automated protocol.
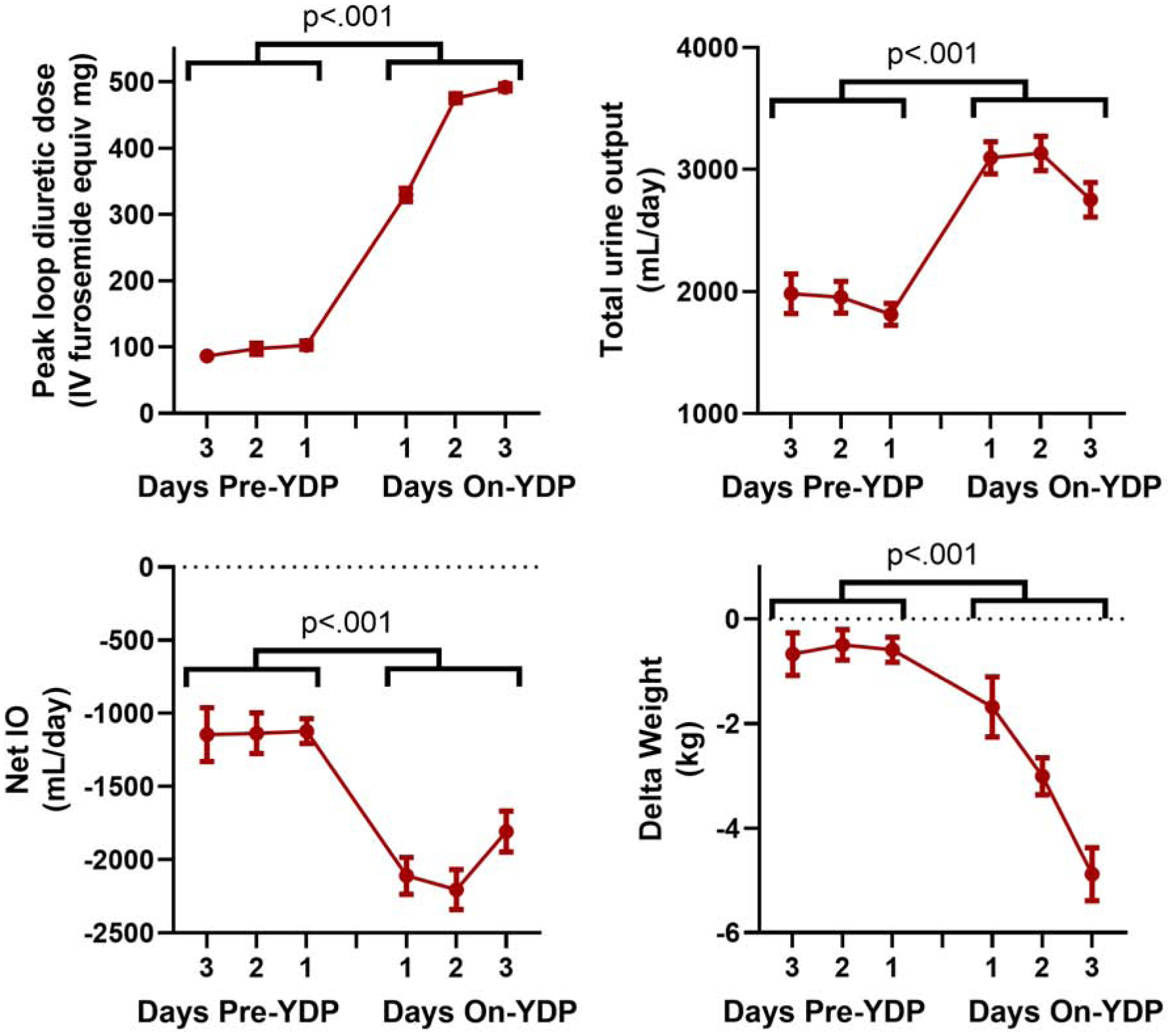
Results: Evaluating 638 loop diuretic administrations, the NRPE showed excellent discrimination with areas under the curve ≥0.90 to predict poor, suboptimal, and excellent natriuretic response, and outperformed clinically obtained net fluid loss (p < 0.05 for all cutpoints). In the YDP cohort (n = 161) using the NRPE to direct therapy mean daily urine output (1.8 ± 0.9 l vs. 3.0 ± 0.8 l), net fluid output (-1.1 ± 0.9 l vs. -2.1 ± 0.9 l), and weight loss (-0.3 ± 0.3 kg vs. -2.5 ± 0.3 kg) improved substantially following initiation of the YDP (p < 0.001 for all pre-post comparisons).
Conclusions: Natriuretic response can be rapidly and accurately predicted by the NRPE, and this information can be used to guide diuretic therapy during acute decompensated heart failure. Additional study of diuresis guided by the NRPE is warranted.
Keywords: diuretics; heart failure; natriuretic response; sodium.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported by National Institutes of Health (NIH) grants K23HL114868, L30HL115790, R01HL139629, R21HL143092, R01HL128973, and R01HL148354 (to Dr. Testani); R01DK113191 and P30DK079210 (to Dr. Wilson); and 5T32HL007950 (to Dr. Griffin). The funding source had no role in study design, data collection, analysis, or interpretation. The contents of this paper are solely the responsibility of the authors and do not necessarily represent the official view of NIH. Dr. Rao has a patent treatment of diuretic resistance (US20200079846A1) issued to Yale and Corvidia Therapeutics Inc. with royalties paid to Yale University; has (with Dr. Testani) a patent method for measuring renalase (WO2019133665A2) issued to Yale; and has received personal fees from Translational Catalyst. Dr. Riello has received consulting fees from Janssen, Johnson & Johnson, Pfizer, and Portola; and has served on advisory boards for AstraZeneca, Janssen, Johnson & Johnson, Medicure, and Portola. Ms. Mahoney has received personal fees from Sequana Medical. Dr. Collins has received grants from the NIH, Patient-Centered Outcomes Research Institute, Agency for Healthcare Research and Quality, and AstraZeneca; and has received personal fees from Ortho Clinical, Boehringer Ingelheim, Roche, and Relypsa Medical. Dr. Testani has (with Dr. Rao) a patent method for measuring renalase (WO2019133665A2) issued to Yale; has received personal fees from Reprieve Medical, AstraZeneca, Novartis, Cardionomic, Bayer, MagentaMed, W.L. Gore, and Windtree Therapeutics; has received grants and personal fees from Bristol Myers Squibb, 3ive Labs, Boehringer Ingelheim, Sanofi, and FIRE1; has received grants from Otsuka, Abbott, and Merck outside of the submitted work; and has patents for treating diuretic resistance filed and issued. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Improving In-Hospital Diuretic Therapy for Heart Failure: The Need for High-Quality Evidence.J Am Coll Cardiol. 2021 Feb 16;77(6):709-712. doi: 10.1016/j.jacc.2020.12.018. J Am Coll Cardiol. 2021. PMID: 33573740 No abstract available.
-
Protocolized Diuretic Approach Using the Natriuretic Equation: Careful Patient Selection Is Needed.J Am Coll Cardiol. 2021 Jun 1;77(21):2757-2758. doi: 10.1016/j.jacc.2021.02.066. J Am Coll Cardiol. 2021. PMID: 34045033 No abstract available.
-
Reply: Protocolized Diuretic Approach Using the Natriuretic Equation: Careful Patient Selection Is Needed.J Am Coll Cardiol. 2021 Jun 1;77(21):2758-2759. doi: 10.1016/j.jacc.2021.03.322. J Am Coll Cardiol. 2021. PMID: 34045035 No abstract available.
References
-
- Gheorghiade M, Filippatos G, De Luca L, Burnett J. Congestion in acute heart failure syndromes: an essential target of evaluation and treatment. Am J Med 2006;119:S3–S10. - PubMed
-
- Gheorghiade M, Follath F, Ponikowski P et al. Assessing and grading congestion in acute heart failure: a scientific statement from the acute heart failure committee of the heart failure association of the European Society of Cardiology and endorsed by the European Society of Intensive Care Medicine. Eur J Heart Fail 2010;12:423–33. - PubMed
-
- Gheorghiade M, Pang PS. Acute heart failure syndromes. J Am Coll Cardiol 2009;53:557–573. - PubMed
-
- Gheorghiade M, Vaduganathan M, Fonarow GC, Bonow RO. Rehospitalization for Heart Failure: Problems and Perspectives. J Am Coll Cardiol 2012. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
