

Progression of Tricuspid Regurgitation After Surgery for Ischemic Mitral Regurgitation
- PMID: 33573741
- PMCID: PMC7953587
- DOI: 10.1016/j.jacc.2020.11.066
Progression of Tricuspid Regurgitation After Surgery for Ischemic Mitral Regurgitation
Abstract
Background: Whether to repair nonsevere tricuspid regurgitation (TR) during surgery for ischemic mitral valve regurgitation (IMR) remains uncertain.
Objectives: The goal of this study was to investigate the incidence, predictors, and clinical significance of TR progression and presence of ≥moderate TR after IMR surgery.
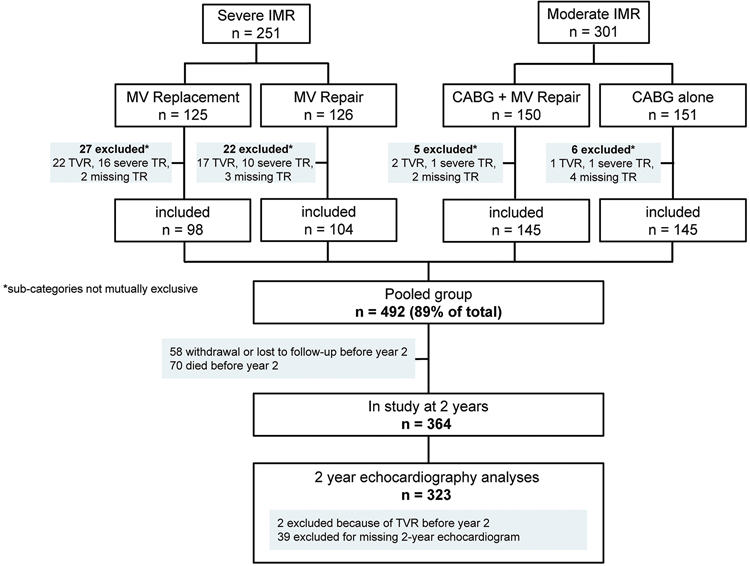
Methods: Patients (n = 492) with untreated nonsevere TR within 2 prospectively randomized IMR trials were included. Key outcomes were TR progression (either progression by ≥2 grades, surgery for TR, or severe TR at 2 years) and presence of ≥moderate TR at 2 years.
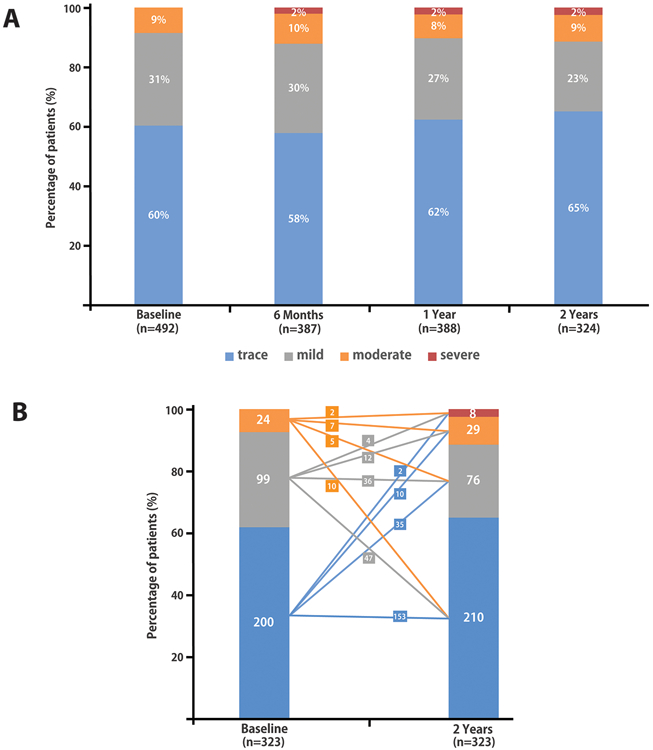
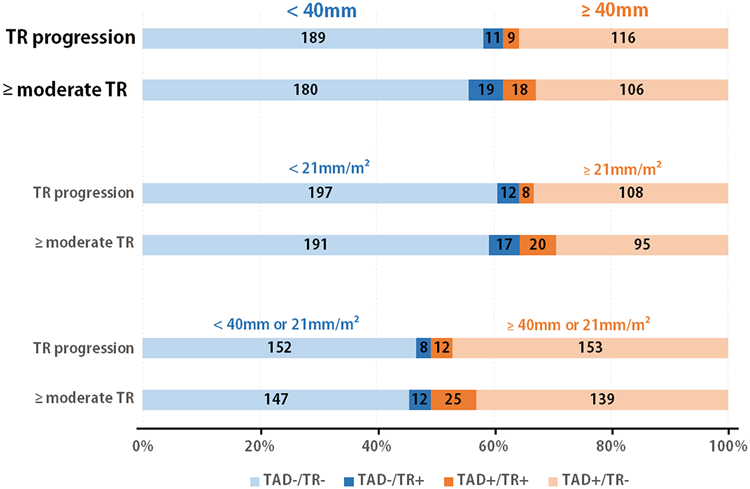
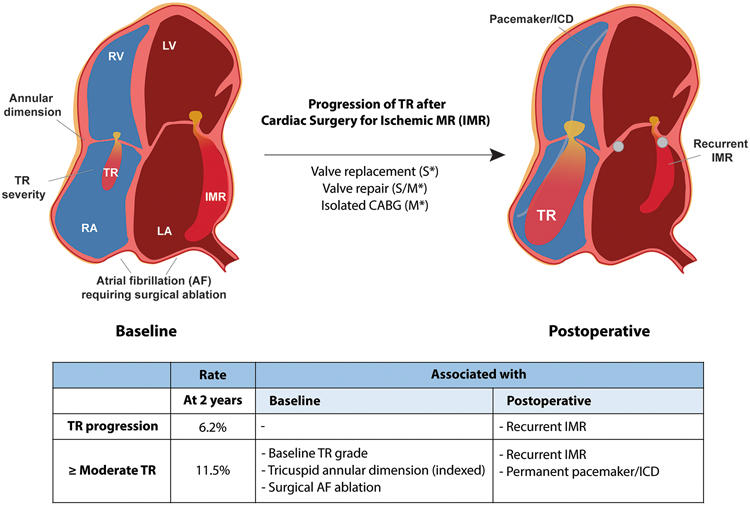
Results: Patients' mean age was 66 ± 10 years (67% male), and TR distribution was 60% ≤trace, 31% mild, and 9% moderate. Among 2-year survivors, TR progression occurred in 20 (6%) of 325 patients. Baseline tricuspid annular diameter (TAD) was not predictive of TR progression. At 2 years, 37 (11%) of 323 patients had ≥moderate TR. Baseline TR grade, indexed TAD, and surgical ablation for atrial fibrillation were independent predictors of ≥moderate TR. However, TAD alone had poor discrimination (area under the curve, ≤0.65). Presence of ≥moderate TR at 2 years was higher in patients with MR recurrence (20% vs. 9%; p = 0.02) and a permanent pacemaker/defibrillator (19% vs. 9%; p = 0.01). Clinical event rates (composite of ≥1 New York Heart Association functional class increase, heart failure hospitalization, mitral valve surgery, and stroke) were higher in patients with TR progression (55% vs. 23%; p = 0.003) and ≥moderate TR at 2 years (38% vs. 22%; p = 0.04).
Conclusions: After IMR surgery, progression of unrepaired nonsevere TR is uncommon. Baseline TAD is not predictive of TR progression and is poorly discriminative of ≥moderate TR at 2 years. TR progression and presence of ≥moderate TR are associated with clinical events. (Comparing the Effectiveness of a Mitral Valve Repair Procedure in Combination With Coronary Artery Bypass Grafting [CABG] Versus CABG Alone in People With Moderate Ischemic Mitral Regurgitation, NCT00806988; Comparing the Effectiveness of Repairing Versus Replacing the Heart's Mitral Valve in People With Severe Chronic Ischemic Mitral Regurgitation, NCT00807040).
Keywords: ischemic heart disease; mitral valve regurgitation; mitral valve surgery; tricuspid annular dilation; tricuspid valve regurgitation.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The Cardiothoracic Surgical Trials Network (CTSN) is supported by a cooperative agreement (U01 HL088942) funded by the National Heart, Lung, and Blood Institute and the National Institute of Neurological Disorders and Stroke of the National Institutes of Health, and the Canadian Institutes for Health Research. The views expressed in this article are those of the authors and do not necessarily represent the views of the National Heart, Lung, and Blood Institute, the National Institute of Neurological Disorders and Stroke, the National Institutes of Health, or the U.S. Department of Health and Human Services. Dr. Ailawadi has received honoraria (modest) from Medtronic, Edwards, Abbott, Admedus, and Gore. Dr. Thourani has served on the Advisory Board (modest) for Gore Vascular; and has received research grants (modest) from Abbott Vascular, Boston Scientific, Edwards Lifesciences, and Jenavalve. Dr. Mack has received honoraria (modest) from Gore; and has received research grants (modest) from Edwards Lifesciences, Medtronic, and Abbott. Dr. Gillinov has served as a consultant (significant) for Medtronic, AtriCure, Edwards Lifesciences, Abbott, CryoLife, and ClearFlow; and has an ownership interest (significant) in ClearFlow. Dr. Giustino has received honoraria (modest) from Bristol Myers Squibb. Dr. O’Gara has been a member of the Executive Committee for the Apollo Trial (TMVR) (modest) for Medtronic; has served as a member of the Executive Committee for the Early TAVR trial (modest) for Edwards Lifesciences; and has served as a member of the Scientific Advisory Board (modest) for MedTrace. Dr. Gammie has served as a consultant (modest) for Edwards Lifesciences. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
The Tricuspid Valve: No Longer Forgotten But Still Not Well Understood.J Am Coll Cardiol. 2021 Feb 16;77(6):725-727. doi: 10.1016/j.jacc.2020.12.012. J Am Coll Cardiol. 2021. PMID: 33573742 No abstract available.
-
Progression of Functional Tricuspid Regurgitation May Be Uncommon After Surgery for Ischemic Mitral Regurgitation: Should the Approach to Concomitant Tricuspid Valve Repair Change?J Cardiothorac Vasc Anesth. 2021 Nov;35(11):3158-3160. doi: 10.1053/j.jvca.2021.05.040. Epub 2021 May 24. J Cardiothorac Vasc Anesth. 2021. PMID: 34172366 No abstract available.
References
-
- Dreyfus GD, Corbi PJ, Chan KM, Bahrami T. Secondary tricuspid regurgitation or dilatation: which should be the criteria for surgical repair? Ann Thorac Surg 2005;79:127–32. - PubMed
-
- David TE, David CM, Manhiolt C. When is tricuspid valve annuloplasty necessary during mitral valve surgery? J Thorac Cardiovasc Surg 2015;150:1043–4. - PubMed
-
- Dion RA. Is the air in Toronto, Rochester, and Cleveland different from that in London, Monaco, Leiden, Genk, Milan, and New York? J Thorac Cardiovasc Surg 2015;150:1040–3. - PubMed
-
- Gillinov M, Mick S, McCurry K, Navia J. The tricuspid valve: If it's not broken, don't fix it. J Thorac Cardiovasc Surg 2017;154:108–109. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:e57–185. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
