

Point-of-care lung ultrasound assessment for risk stratification and therapy guiding in COVID-19 patients: a prospective noninterventional study
- PMID: 33574074
- PMCID: PMC7877323
- DOI: 10.1183/13993003.04283-2020
Point-of-care lung ultrasound assessment for risk stratification and therapy guiding in COVID-19 patients: a prospective noninterventional study
Abstract
Background: Lung ultrasound is feasible for assessing lung injury caused by coronavirus disease 2019 (COVID-19). However, the prognostic meaning and time-line changes of lung injury assessed by lung ultrasound in COVID-19 hospitalised patients are unknown.
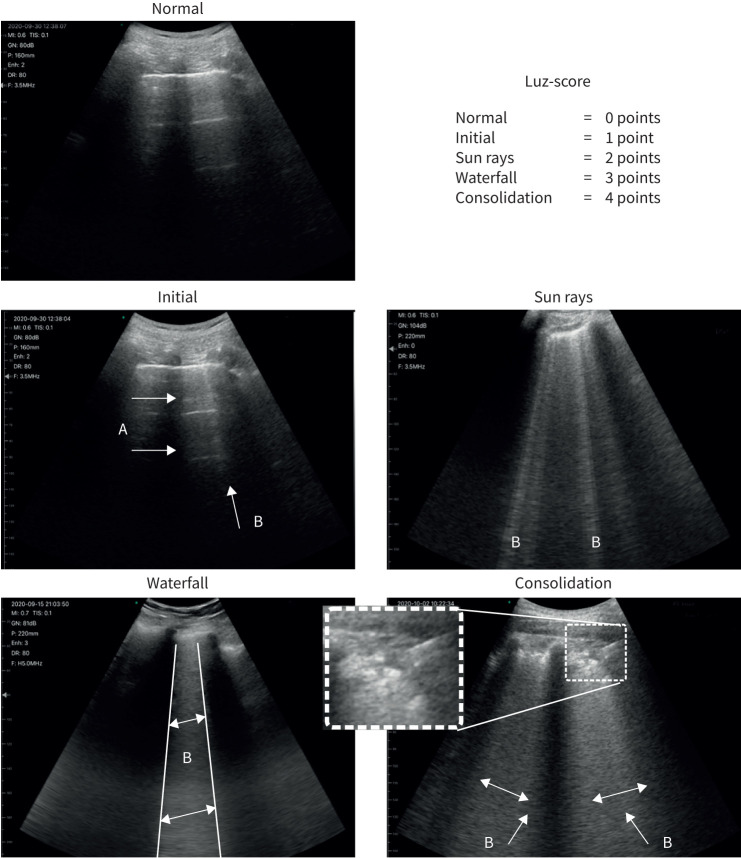
Methods: Prospective cohort study designed to analyse prognostic value of lung ultrasound in COVID-19 patients by using a quantitative scale (lung ultrasound Zaragoza (LUZ)-score) during the first 72 h after admission. The primary end-point was in-hospital death and/or admission to the intensive care unit. Total length of hospital stay, increase of oxygen flow and escalation of medical treatment during the first 72 h were secondary end-points.
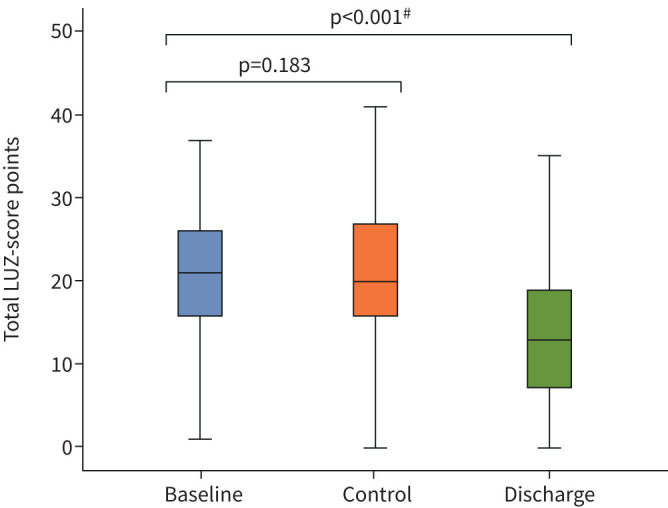
Results: 130 patients were included in the final analysis; mean±sd age was 56.7±13.5 years. Median (interquartile range) time from the beginning of symptoms to admission was 6 (4-9) days. Lung injury assessed by LUZ-score did not differ during the first 72 h (21 (16-26) points at admission versus 20 (16-27) points at 72 h; p=0.183). In univariable logistic regression analysis, estimated arterial oxygen tension/inspiratory oxygen fraction ratio (PAFI) (hazard ratio 0.99, 95% CI 0.98-0.99; p=0.027) and LUZ-score >22 points (5.45, 1.42-20.90; p=0.013) were predictors for the primary end-point.
Conclusions: LUZ-score is an easy, simple and fast point-of-care ultrasound tool to identify patients with severe lung injury due to COVID-19, upon admission. Baseline score is predictive of severity along the whole period of hospitalisation. The score facilitates early implementation or intensification of treatment for COVID-19 infection. LUZ-score may be combined with clinical variables (as estimated by PAFI) to further refine risk stratification.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: J. Rubio-Gracia has nothing to disclose. Conflict of interest: I. Giménez-López has nothing to disclose. Conflict of interest: V. Garcés-Horna has nothing to disclose. Conflict of interest: D. López-Delgado has nothing to disclose. Conflict of interest: J.L. Sierra-Monzón has nothing to disclose. Conflict of interest: L. Martínez-Lostao has nothing to disclose. Conflict of interest: C. Josa-Laorden has nothing to disclose. Conflict of interest: F. Ruiz-Laiglesia has nothing to disclose. Conflict of interest: J.I. Pérez-Calvo has nothing to disclose. Conflict of interest: S. Crespo-Aznarez has nothing to disclose. Conflict of interest: J. García-Lafuente has nothing to disclose. Conflict of interest: N. Peña-Fresneda has nothing to disclose. Conflict of interest: B. Amores Arriaga has nothing to disclose. Conflict of interest: B. Gracia-Tello has nothing to disclose. Conflict of interest: M. Sánchez-Marteles has nothing to disclose.
Figures
Similar articles
-
Multiple Approaches at Admission Based on Lung Ultrasound and Biomarkers Improves Risk Identification in COVID-19 Patients.J Clin Med. 2021 Nov 23;10(23):5478. doi: 10.3390/jcm10235478. J Clin Med. 2021. PMID: 34884180 Free PMC article.
-
Point-of-Care Lung Ultrasound for COVID-19: Findings and Prognostic Implications From 105 Consecutive Patients.J Intensive Care Med. 2021 Mar;36(3):334-342. doi: 10.1177/0885066620988831. J Intensive Care Med. 2021. PMID: 33535883 Free PMC article.
-
Comparative analysis of chest radiography and lung ultrasound to predict intra-hospital prognosis of patients admitted for acute SARS-CoV-2 pneumonia (COVID-19).Med Clin (Barc). 2022 Dec 9;159(11):515-521. doi: 10.1016/j.medcli.2022.01.028. Epub 2022 Mar 3. Med Clin (Barc). 2022. PMID: 35428513 Free PMC article. English, Spanish.
-
Prognostic value of bedside lung ultrasound score in patients with COVID-19.Crit Care. 2020 Dec 22;24(1):700. doi: 10.1186/s13054-020-03416-1. Crit Care. 2020. PMID: 33353548 Free PMC article.
-
Subcutaneous Sarilumab in hospitalised patients with moderate-severe COVID-19 infection compared to the standard of care (SARCOVID): a structured summary of a study protocol for a randomised controlled trial.Trials. 2020 Sep 9;21(1):772. doi: 10.1186/s13063-020-04588-5. Trials. 2020. PMID: 32907638 Free PMC article.
Cited by
-
Past and Present of Point-of-Care Ultrasound (PoCUS): A Narrative Review.Cureus. 2023 Dec 8;15(12):e50155. doi: 10.7759/cureus.50155. eCollection 2023 Dec. Cureus. 2023. PMID: 38192958 Free PMC article. Review.
-
Multiple Approaches at Admission Based on Lung Ultrasound and Biomarkers Improves Risk Identification in COVID-19 Patients.J Clin Med. 2021 Nov 23;10(23):5478. doi: 10.3390/jcm10235478. J Clin Med. 2021. PMID: 34884180 Free PMC article.
-
Point-of-care ultrasonography for risk stratification of non-critical suspected COVID-19 patients on admission (POCUSCO): A prospective binational study.PLoS One. 2023 Apr 26;18(4):e0284748. doi: 10.1371/journal.pone.0284748. eCollection 2023. PLoS One. 2023. PMID: 37099493 Free PMC article.
-
Lung ultrasound score and in-hospital mortality of adults with acute respiratory distress syndrome: a meta-analysis.BMC Pulm Med. 2024 Jan 29;24(1):62. doi: 10.1186/s12890-023-02826-5. BMC Pulm Med. 2024. PMID: 38287299 Free PMC article.
-
Role of Lung Ultrasound in the Management of Patients with Suspected SARS-CoV-2 Infection in the Emergency Department.J Clin Med. 2022 Apr 7;11(8):2067. doi: 10.3390/jcm11082067. J Clin Med. 2022. PMID: 35456160 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical