

Morpho-functional changes of cardiac telocytes in isolated atrial amyloidosis in patients with atrial fibrillation
- PMID: 33574429
- PMCID: PMC7878494
- DOI: 10.1038/s41598-021-82554-0
Morpho-functional changes of cardiac telocytes in isolated atrial amyloidosis in patients with atrial fibrillation
Abstract
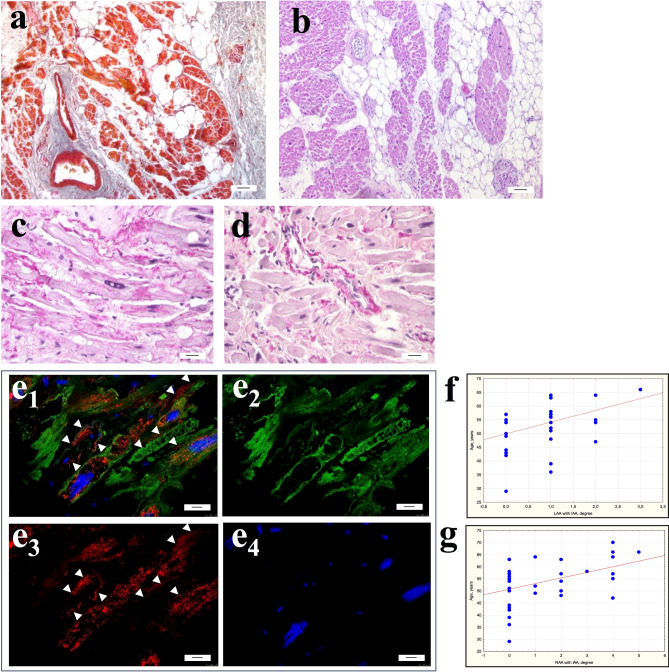
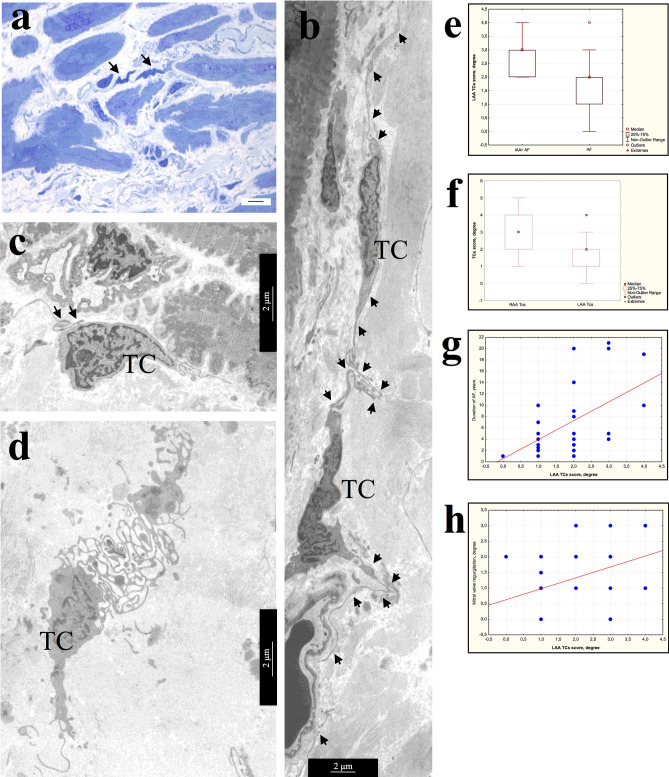
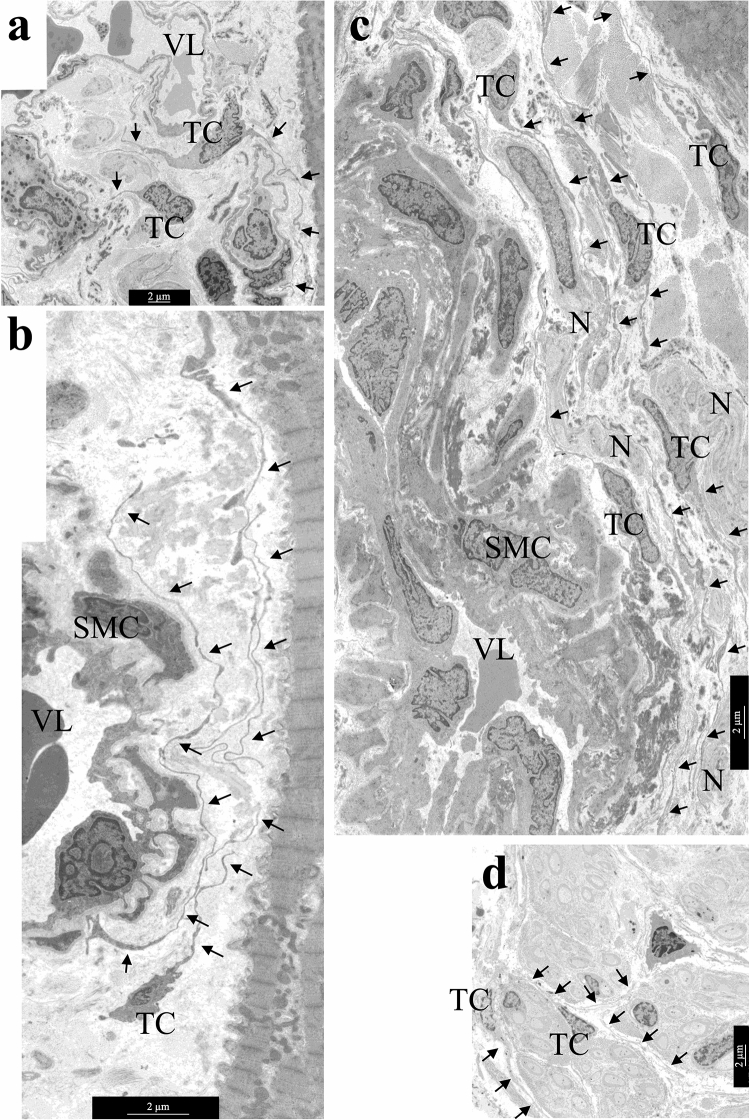
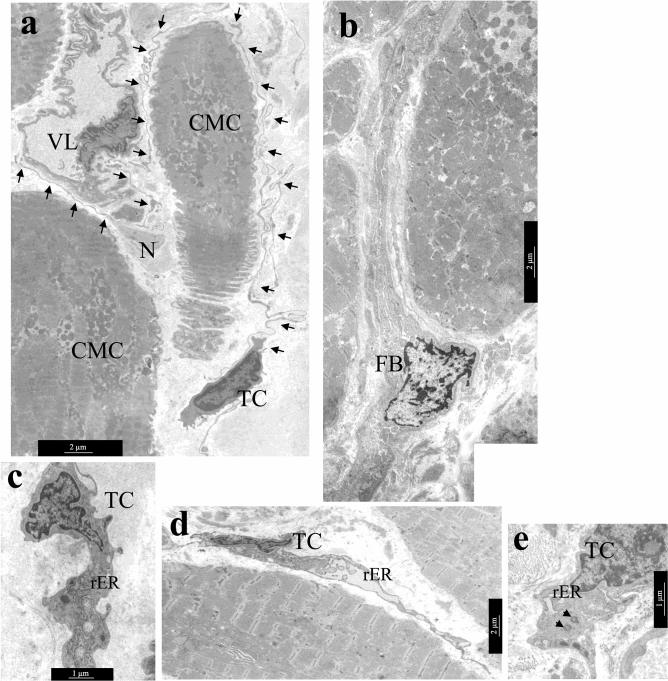
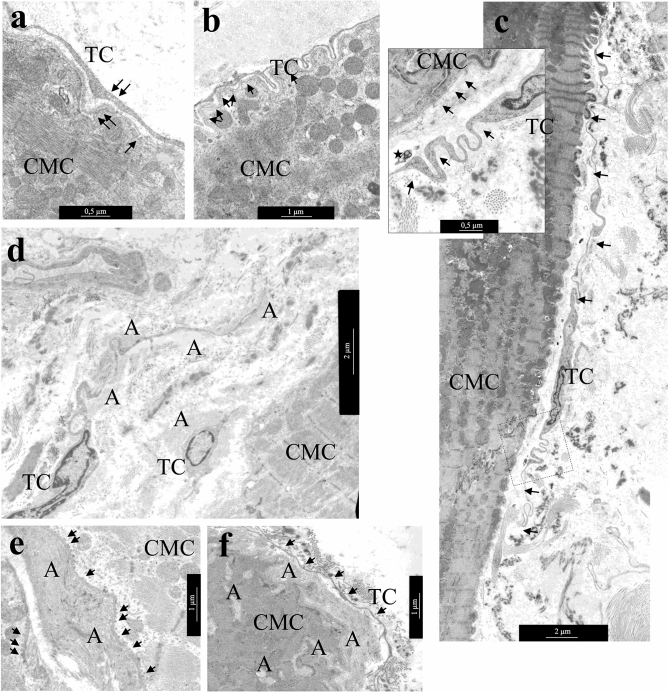
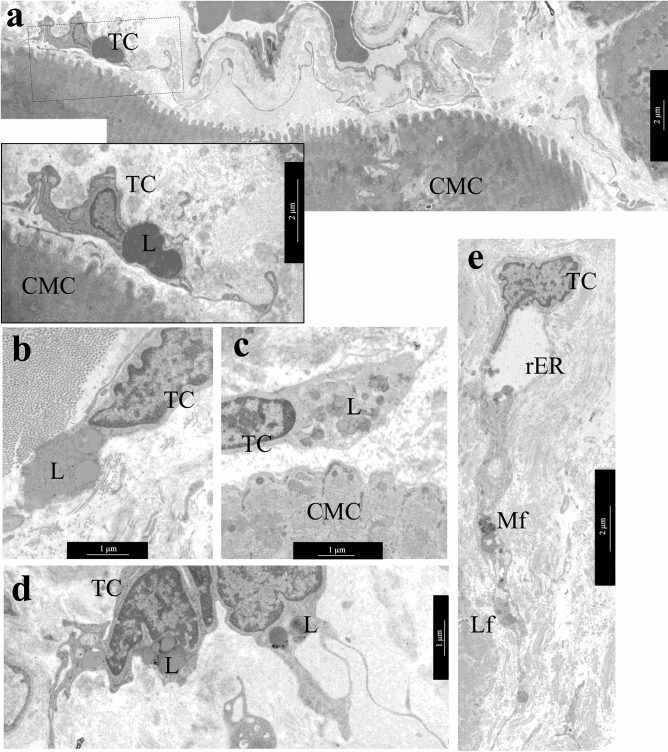
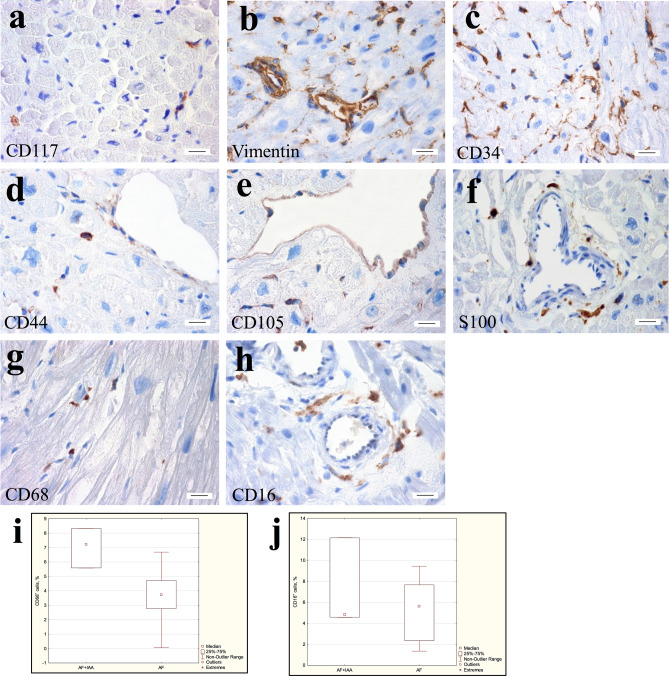
Telocytes are interstitial cells with long, thin processes by which they contact each other and form a network in the interstitium. Myocardial remodeling of adult patients with different forms of atrial fibrillation (AF) occurs with an increase in fibrosis, age-related isolated atrial amyloidosis (IAA), cardiomyocyte hypertrophy and myolysis. This study aimed to determine the ultrastructural and immunohistochemical features of cardiac telocytes in patients with AF and AF + IAA. IAA associated with accumulation of atrial natriuretic factor was detected in 4.3-25% biopsies of left (LAA) and 21.7-41.7% of right (RAA) atrial appendage myocardium. Telocytes were identified at ultrastructural level more often in AF + IAA, than in AF group and correlated with AF duration and mitral valve regurgitation. Telocytes had ultrastructural signs of synthetic, proliferative, and phagocytic activity. Telocytes corresponded to CD117+, vimentin+, CD34+, CD44+, CD68+, CD16+, S100-, CD105- immunophenotype. No significant differences in telocytes morphology and immunophenotype were found in patients with various forms of AF. CD68-positive cells were detected more often in AF + IAA than AF group. We assume that in aged AF + IAA patients remodeling of atrial myocardium provoked transformation of telocytes into "transitional forms" combining the morphological and immunohistochemical features with signs of fibroblast-, histiocyte- and endotheliocyte-like cells.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
