

An updated meta-analysis of MitraClip versus surgery for mitral regurgitation
- PMID: 33575171
- PMCID: PMC7867427
- DOI: 10.21037/acs-2020-mv-24
An updated meta-analysis of MitraClip versus surgery for mitral regurgitation
Abstract
Background: Although studies demonstrate its feasibility, there is ongoing debate on the short and long-term outcomes of MitraClip versus surgical repair or mitral valve replacement (MVR). The objective of this meta-analysis is to compare the safety, morbidity, mortality and long-term function following MitraClip compared to MVR.
Methods: Articles were searched in PubMed and Cochrane databases for studies comparing outcomes of MitraClip and surgery on December 1, 2019. Eligible prospective, retrospective, randomized and non-randomized studies were reviewed.
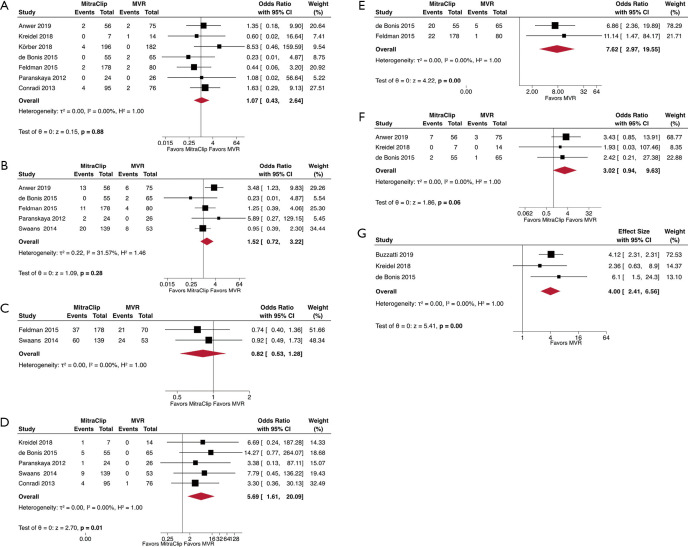
Results: A total of nine studies (n=1,873, MitraClip =533, MVR =644) were eligible for review. At baseline, MitraClip patients had more comorbidities than MVR patients, including myocardial infarction (P<0.001), chronic obstructive pulmonary disease (P=0.022) and chronic kidney disease (P<0.001). MitraClip was associated with shorter length of stay (-3.86 days; 95% CI, -4.73 to -2.99; P<0.01) with a similar safety profile. Residual moderate-to-severe mitral regurgitation was more frequent in MitraClip at discharge (OR, 2.81; 95% CI, 1.39-5.69; P<0.01) and at five years (OR, 2.46; 95% CI, 1.54-3.94; P<0.01), and there was a higher need for reoperation on the MitraClip group at latest follow-up (OR, 5.28; 95% CI, 3.43-8.11; P<0.01). The overall mortality was comparable between the two groups (HR, 2.06; 95% CI, 0.98-4.29; P=0.06) for a mean follow-up of 4.8 years.
Conclusions: Compared to surgery, MitraClip demonstrates a similar safety profile and shorter length of stay in high-risk patients, at the expense of increased residual mitral regurgitation and higher reoperation rate. Despite this, long term mortality appears comparable between the two techniques, suggesting that a patient-tailored approach will lead to optimal results.
Keywords: MitraClip; mitral regurgitation (MR); mitral valve (MV); mitral valve repair.
2021 Annals of Cardiothoracic Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures




References
LinkOut - more resources
Full Text Sources
Other Literature Sources