

Severity of early allograft dysfunction following donation after circulatory death liver transplantation: a multicentre study
- PMID: 33575286
- PMCID: PMC7867715
- DOI: 10.21037/hbsn.2019.09.02
Severity of early allograft dysfunction following donation after circulatory death liver transplantation: a multicentre study
Abstract
Background: Early allograft dysfunction (EAD) is associated with decreased graft and patient survival rates. This study aimed to identify the severity of EAD and develop a predictive model for EAD after donation after circulatory death (DCD) liver transplantation (LT). Furthermore, the influence of operative time on EAD incidence was also evaluated.
Methods: In this retrospective, multicentre cohort study, nomograms were established based on a single-centre training cohort (n=321) and validated in a 3-center validation cohort (n=501).
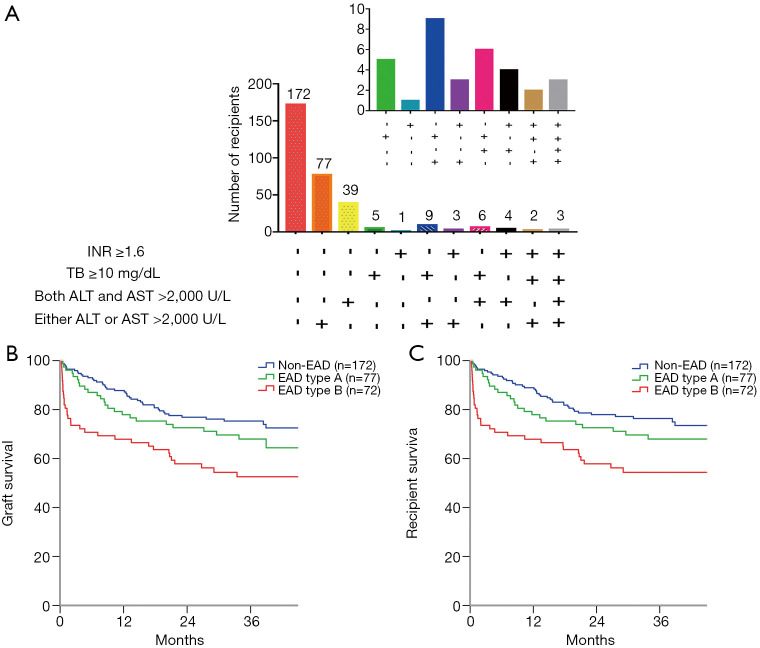
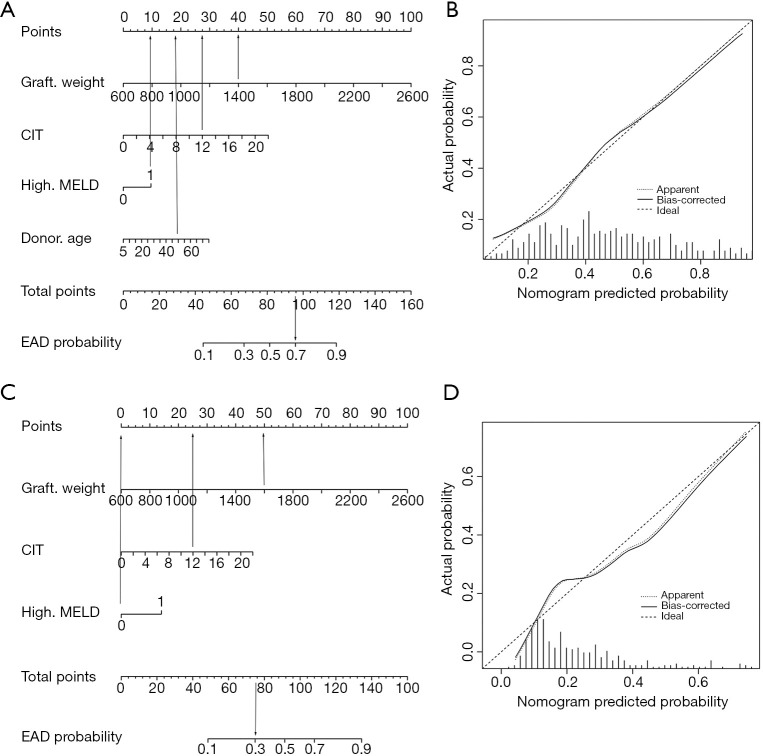
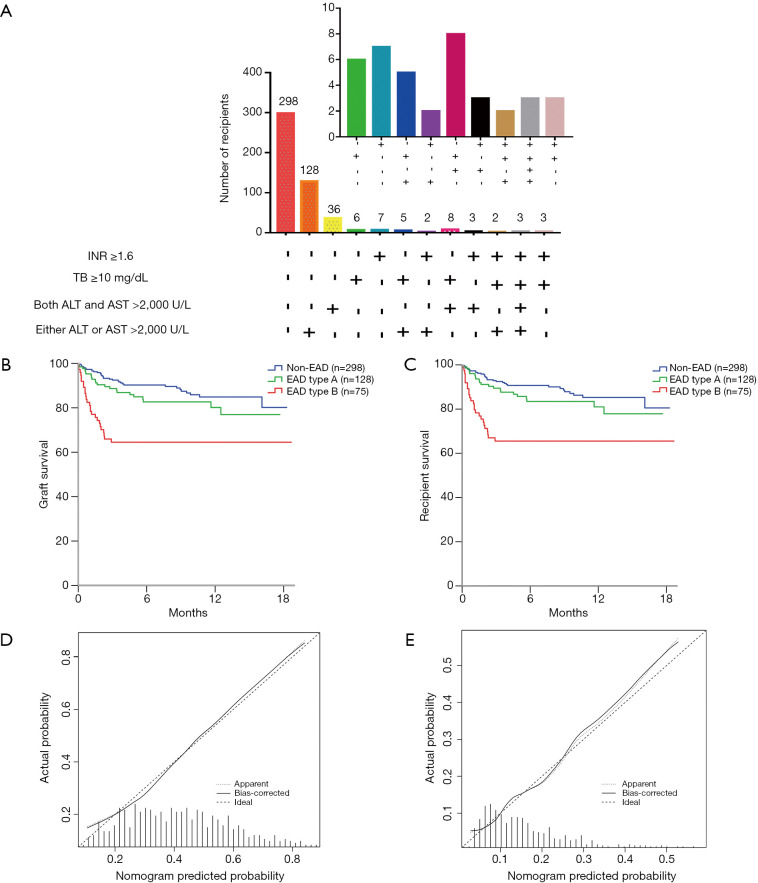
Results: The incidence rate of EAD was 46.4% (149/321) in the training cohort and 40.5% (203/501) in the validation cohort. Of the 149 EAD patients in the training cohort, 77 patients with either elevated alanine aminotransferase (ALT) or aspartate aminotransferase (AST) were classified as having EAD type A, and the rest of the EAD patients were classified as having EAD type B. Recipients with EAD type B had lower graft and patient survival rates than recipients with EAD type A (P=0.043 and 0.044, respectively). We further developed a nomogram to predict EAD (graft weight, cold ischemia time, donor age, model for end-stage liver disease (MELD) score) and another nomogram to predict EAD type B (graft weight, cold ischemia time, MELD score). The nomograms for the prediction of EAD and EAD type B had good discrimination [concordance index (C-index) =0.712 (0.666-0.758), 0.707 (0.641-0.773)] and calibration [Hosmer-Lemeshow (HL) P=0.384, P=0.425] in the validation cohort. An increased operative time (>6 h) was associated with increased EAD and EAD type B incidence in the high-risk group (P=0.005, P=0.020, respectively).
Conclusions: EAD type B was associated with decreased graft and patient survival rates. The novel nomograms effectively predicted the incidence of EAD and EAD type B in DCD LT patients.
Keywords: Liver transplantation; donation after circulatory death; early allograft dysfunction (EAD).
2021 Hepatobiliary Surgery and Nutrition. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/hbsn.2019.09.02). The authors have no conflicts of interest to declare.
Figures
References
-
- Okamura Y, Yagi S, Sato T, et al. Coexistence of Bilirubin ≥10 mg/dL and Prothrombin Time-International Normalized Ratio ≥1.6 on Day 7: A Strong Predictor of Early Graft Loss After Living Donor Liver Transplantation. Transplantation 2018;102:440-7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources