

Association between Frailty and Mortality, Falls, and Hospitalization among Patients with Hypertension: A Systematic Review and Meta-Analysis
- PMID: 33575325
- PMCID: PMC7861941
- DOI: 10.1155/2021/2690296
Association between Frailty and Mortality, Falls, and Hospitalization among Patients with Hypertension: A Systematic Review and Meta-Analysis
Abstract
Objective: Chronological age alone does not adequately reflect the difference in health status of a patient with hypertension. Frailty is closely associated with biological age, and its assessment is clinically useful in addressing the heterogeneity of health status. The purpose of our study is to comprehensively examine the predictive value of frailty for negative health outcomes in hypertensive patients through a systematic review and meta-analysis.
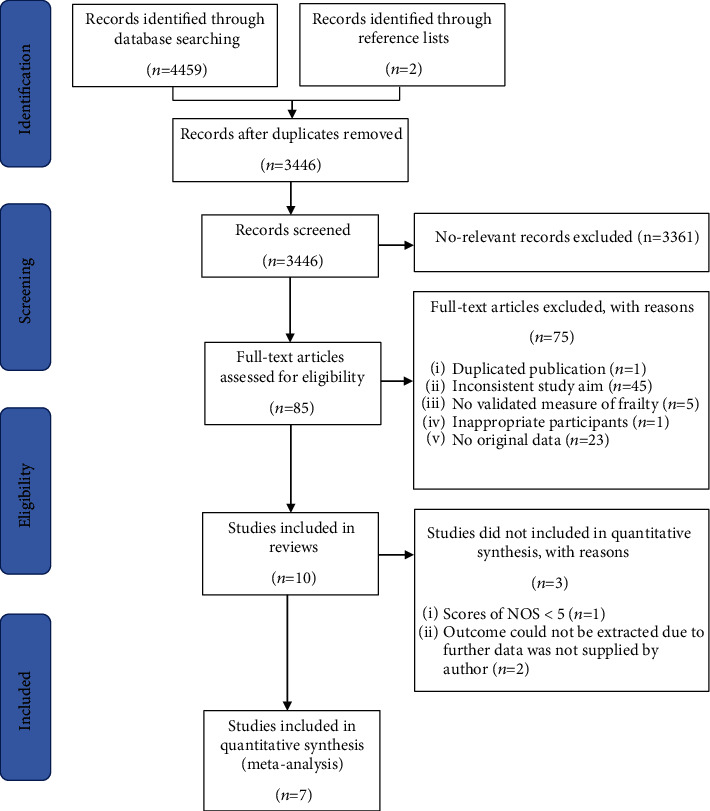
Methods: Multiple English and Chinese databases were searched from inception to 04.11.2020. All cross-sectional and longitudinal studies that examined the association between frailty and relevant clinical outcomes among hypertensive patients were included. The NOS was used to assess the risk of bias of studies included in the analysis. Hazard ratios (HRs), odds ratios (ORs), and 95% confidence intervals (CIs) were pooled for outcomes associated with frailty.
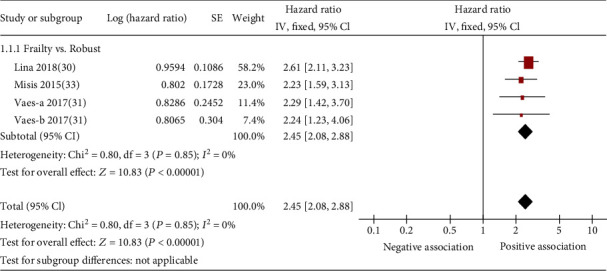
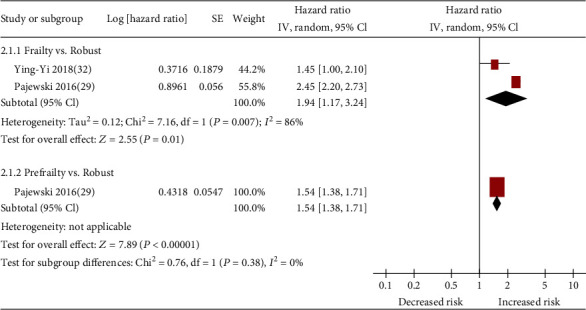
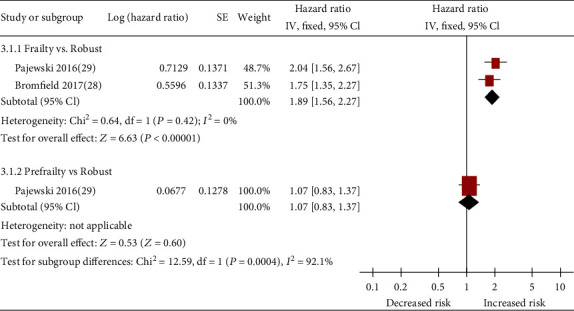
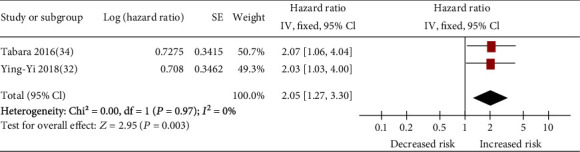
Results: Six longitudinal studies and one cross-sectional study involving 17403 patients with hypertension were included in the meta-analysis. The risk of bias of all included studies was rated as low or moderate. The pooled HR of frailty related to mortality was 2.45 (95% CI: 2.08-2.88). The pooled HR of prefrailty and frailty-related injurious falls was 1.07 (95% CI: 0.83-1.37) and 1.89 (95% CI: 1.56-2.27), respectively. The pooled HR of prefrailty and frailty-related hospitalization was 1.54 (95% CI: 1.38-1.71) and 1.94 (95% CI: 1.17-3.24), respectively.
Conclusions: This systematic review suggests that frailty was a strong predictor of mortality, hospitalization, and injurious falls among patients with hypertension. Our findings indicate that assessment of frailty in patients with hypertension to guide their management may be necessary in clinical setting. However, our finding was based on very limited amount studies; thus, future studies are required to further validate the role of frailty in prediction of negative health outcomes in hypertensive patients as well as pay more attention to the following knowledge gaps: (1) the association between frailty and hypertension-related outcomes, (2) the significance of the association between different frailty models and relevant clinical outcomes, and (3) the predictive value of prefrailty for the negative health outcomes in people with hypertension.
Copyright © 2021 Kaiyan Hu et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Frailty as a Predictor of Negative Health Outcomes in Chronic Kidney Disease: A Systematic Review and Meta-Analysis.J Am Med Dir Assoc. 2021 Mar;22(3):535-543.e7. doi: 10.1016/j.jamda.2020.09.033. Epub 2020 Nov 18. J Am Med Dir Assoc. 2021. PMID: 33218914
-
Association between frailty and adverse outcomes in patients undergoing maintenance hemodialysis: a systematic review and meta-analysis.Ren Fail. 2024 Dec;46(2):2367716. doi: 10.1080/0886022X.2024.2367716. Epub 2024 Aug 5. Ren Fail. 2024. PMID: 39099468 Free PMC article.
-
Frailty as a predictor of future falls in hospitalized patients: A systematic review and meta-analysis.Geriatr Nurs. 2020 Mar-Apr;41(2):69-74. doi: 10.1016/j.gerinurse.2019.01.004. Epub 2019 Feb 11. Geriatr Nurs. 2020. PMID: 30765177
-
Motoric Cognitive Risk Syndrome as a Predictor of Adverse Health Outcomes: A Systematic Review and Meta-Analysis.Gerontology. 2024;70(7):669-688. doi: 10.1159/000538314. Epub 2024 May 2. Gerontology. 2024. PMID: 38697041
-
Relationship between frailty and mortality, hospitalization, and cardiovascular diseases in diabetes: a systematic review and meta-analysis.Cardiovasc Diabetol. 2019 Jun 18;18(1):81. doi: 10.1186/s12933-019-0885-2. Cardiovasc Diabetol. 2019. PMID: 31215496 Free PMC article.
Cited by
-
Correlates of Frailty in Hospitalized Older Adults with Hypertension and Its Influence on Clinical Prognosis.Int J Gen Med. 2024 Aug 2;17:3373-3385. doi: 10.2147/IJGM.S465973. eCollection 2024. Int J Gen Med. 2024. PMID: 39113783 Free PMC article.
-
Hypertension in frail older adults: current perspectives.PeerJ. 2024 Jul 11;12:e17760. doi: 10.7717/peerj.17760. eCollection 2024. PeerJ. 2024. PMID: 39006023 Free PMC article. Review.
-
Hypertension Treatment in Frail Older Adults: A Systematic Review and Appraisal of Guidelines.Drugs Aging. 2023 Oct;40(10):881-893. doi: 10.1007/s40266-023-01053-1. Epub 2023 Aug 18. Drugs Aging. 2023. PMID: 37594718
-
Physiological Systems in Promoting Frailty.Compr Physiol. 2022 Apr 26;12(3):3575-3620. doi: 10.1002/cphy.c210034. Compr Physiol. 2022. PMID: 35578945 Free PMC article. Review.
-
Frailty, All-Cause Mortality, and Hospitalization in Patients on Maintenance Hemodialysis: A Systematic Review and Meta-Analysis.J Clin Med. 2025 Jul 10;14(14):4914. doi: 10.3390/jcm14144914. J Clin Med. 2025. PMID: 40725607 Free PMC article. Review.
References
-
- World Health Organization. A global brief on hypertension: silent killer, global public health crisis. Geneva, Switzerland: 2013. (World Health Day 2013 Report).
-
- Beckett N., Peters R., Tuomilehto J., et al. Immediate and late benefits of treating very elderly people with hypertension: results from active treatment extension to Hypertension in the Very Elderly randomised controlled trial. BMJ. 2012;344:d7541–d7541. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
