

A systematic review and meta-analysis of laparotomy compared with laparoscopic management of interstitial pregnancy
- PMID: 33575679
- PMCID: PMC7863690
A systematic review and meta-analysis of laparotomy compared with laparoscopic management of interstitial pregnancy
Abstract
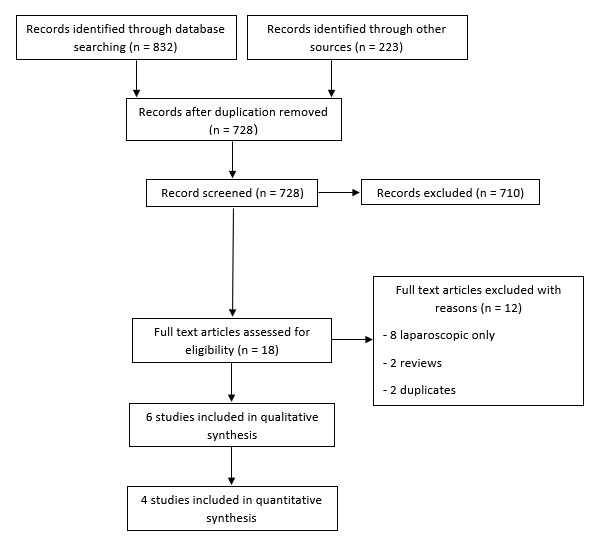
Background: Interstitial pregnancy is a rare but life-threatening condition accounting for 1-4% of all types of tubal ectopic pregnancies. It can be managed by open and minimally invasive surgical techniques. Our goal was to compare laparoscopic and open surgery for managing interstitial pregnancy.
Search strategy: We searched PubMed, Scopus, Web of Science, and Cochrane up to May 2020.
Selection criteria: 1) Women with interstitial pregnancy, 2) Intervention: laparoscopic surgery, 3) Comparator: open surgery, 4) Outcomes: Hospital stay, operation time, pain scale, blood loss. Secondary outcomes: any other reported 5) Study designs: interventional and observational.
Data collection and analysis: Data was extracted from the relevant articles and was pooled as mean difference (MD) or relative risk (RR) with a 95% confidence interval (CI).
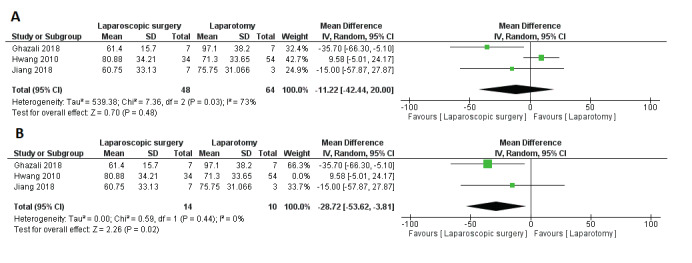
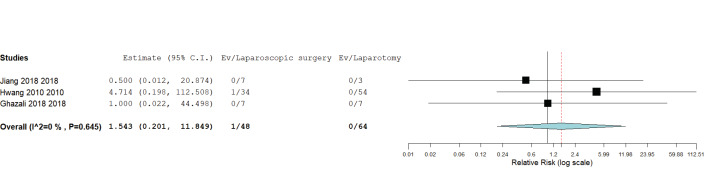
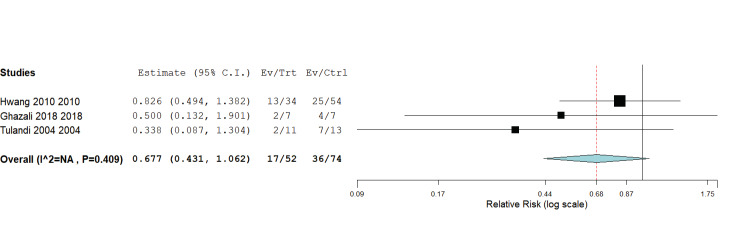
Main results: We included six studies, three of which provided eligible data. The duration of hospital stay was lower in the laparoscopic surgery group (MD = -1.42, 95% CI [-1.72, -0.76], P < 0.0001). There was no significant difference in operative time (MD = 5.90, 95% CI [-11.30, 23.09], P = 0.50, blood loss (MD = -9.43, 95% CI [-214.18, 195.32], P = 0.93), complications (RR = 1.54, 95% CI [0.20, 11.85], P = 0.68), or blood transfusions (RR = 0.77, 95% CI [0.50, 1.25], P = 0.30).
Conclusion: Laparoscopic surgery is associated with shorter hospital stay, with no difference in terms of blood loss, post-, and intraoperative complications, and need for blood transfusion compared with laparotomy.
Keywords: Interstitial pregnancy; cornual; ectopic; laparoscopy; laparotomy; meta-analysis.
Copyright © 2020 Facts, Views & Vision.
Conflict of interest statement
Conflicts of Interest:Authors declare no conflicts of interest.
Figures


References
-
- Bremner T, Cela V, Luciano AA. Surgical management of interstitial pregnancy. J Minim Invasive Gynecol. 2000;7(3):387–389. - PubMed
-
- Chan LY-S, Yuen PM. Successful treatment of ruptured interstitial pregnancy with laparoscopic surgery: A report of 2 cases. J REPROD MED. 2003;48:569–571. - PubMed
-
- Cucinella G, Calagna G, Rotolo S, et al. Interstitial pregnancy: A ‘Road Map’ of surgical treatment based on a systematic review of the literature. Gynecol Obstet Invest. 2014;78:141–149. - PubMed
-
- Diagnosis and Management of Ectopic Pregnancy: Green-top Guideline No. 21. BJOG. 2016;123:15–55. - PubMed
Publication types
LinkOut - more resources
Full Text Sources