

Diagnostic accuracy of physician's gestalt in suspected COVID-19: Prospective bicentric study
- PMID: 33576155
- PMCID: PMC8014604
- DOI: 10.1111/acem.14232
Diagnostic accuracy of physician's gestalt in suspected COVID-19: Prospective bicentric study
Abstract
Objectives: Physicians' gestalt is central in the diagnostic pipeline of suspected COVID-19, due to the absence of a single tool allowing conclusive rule in or rule out. The aim of this study was to estimate the diagnostic test characteristics of physician's gestalt for COVID-19 in the emergency department (ED), based on clinical findings or on a combination of clinical findings and bedside imaging results.
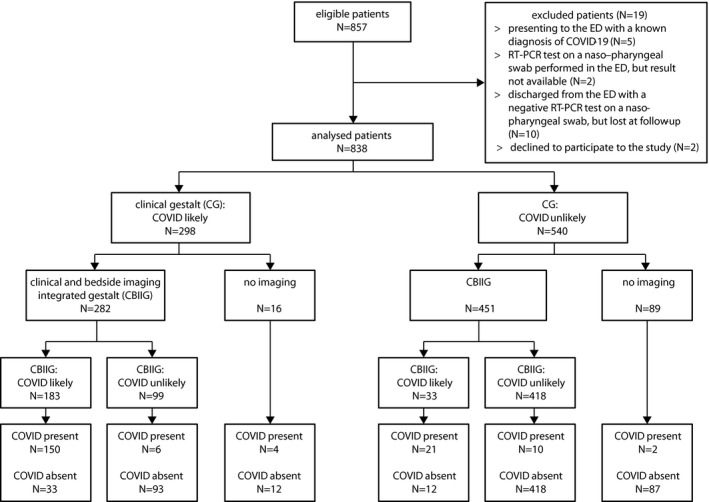
Methods: From April 1 to April 30, 2020, patients with suspected COVID-19 were prospectively enrolled in two EDs. Physicians prospectively dichotomized patients in COVID-19 likely or unlikely twice: after medical evaluation of clinical features (clinical gestalt [CG]) and after evaluation of clinical features and results of lung ultrasound or chest x-ray (clinical and bedside imaging-integrated gestalt [CBIIG]). The final diagnosis was adjudicated after independent review of 30-day follow-up data.
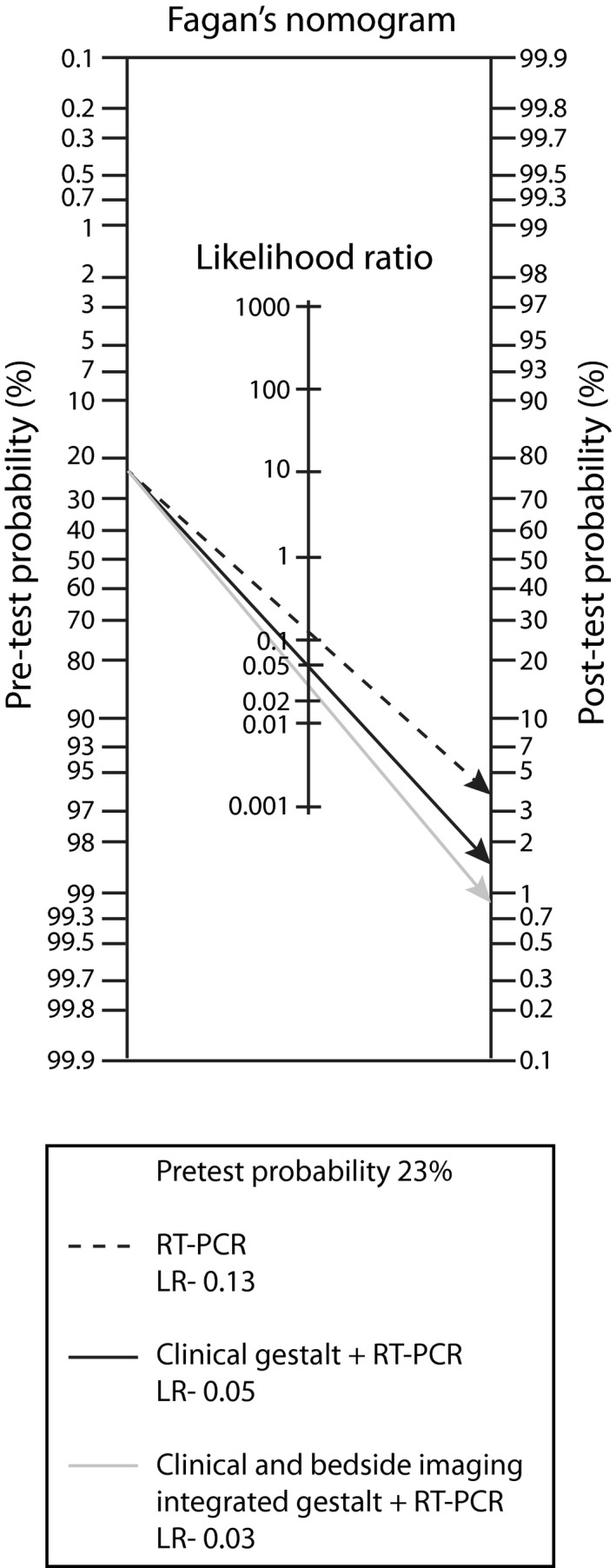
Results: Among 838 ED enrolled patients, 193 (23%) were finally diagnosed with COVID-19. The area under the curve (AUC), sensitivity, and specificity of CG and CBIIG for COVID-19 were 80.8% and 91.6% (p < 0.01), 82.9% and 91.4% (p = 0.01), and 78.6% and 91.8% (p < 0.01), respectively. CBIIG had similar AUC and sensitivity to reverse transcription-polymerase chain reaction (RT-PCR) for SARS-CoV-2 on the first nasopharyngeal swab per se (93.5%, p = 0.24; and 87%, p = 0.17, respectively). CBIIG plus RT-PCR had a sensitivity of 98.4% for COVID-19 (p < 0.01 vs. RT-PCR alone) compared to 95.9% for CG plus RT-PCR (p = 0.05).
Conclusions: In suspected COVID-19, CG and CBIIG have fair diagnostic accuracy, in line with physicians' gestalt for other acute conditions. Negative RT-PCR plus low probability based on CBIIG can rule out COVID-19 with a relatively low number of false-negative cases.
Keywords: COVID-19; diagnosis; emergency department; gestalt; lung ultrasound chest x-ray.
© 2021 by the Society for Academic Emergency Medicine.
Conflict of interest statement
The authors have no potential conflicts to disclose.
Figures
Similar articles
-
Inter-rater reliability and prospective validation of a clinical prediction rule for SARS-CoV-2 infection.Acad Emerg Med. 2021 Jul;28(7):761-767. doi: 10.1111/acem.14309. Epub 2021 Jun 21. Acad Emerg Med. 2021. PMID: 34133794 Free PMC article.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Sep 30;9:CD013639. doi: 10.1002/14651858.CD013639.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. PMID: 32997361 Updated.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Mar 16;3:CD013639. doi: 10.1002/14651858.CD013639.pub4. PMID: 33242342 Updated.
-
Chest CT in patients with a moderate or high pretest probability of COVID-19 and negative swab.Radiol Med. 2020 Dec;125(12):1260-1270. doi: 10.1007/s11547-020-01269-w. Epub 2020 Aug 29. Radiol Med. 2020. PMID: 32862406 Free PMC article.
-
A Computational Approach in the Diagnostic Process of COVID-19: The Missing Link between the Laboratory and Emergency Department.Front Biosci (Landmark Ed). 2023 Feb 22;28(2):31. doi: 10.31083/j.fbl2802031. Front Biosci (Landmark Ed). 2023. PMID: 36866553
Cited by
-
Inter-rater reliability and prospective validation of a clinical prediction rule for SARS-CoV-2 infection.Acad Emerg Med. 2021 Jul;28(7):761-767. doi: 10.1111/acem.14309. Epub 2021 Jun 21. Acad Emerg Med. 2021. PMID: 34133794 Free PMC article.
-
Ability of emergency medicine clinicians to predict COVID-19 in their patients.Am J Emerg Med. 2022 Jun;56:329-331. doi: 10.1016/j.ajem.2021.09.001. Epub 2021 Sep 3. Am J Emerg Med. 2022. PMID: 34509327 Free PMC article. No abstract available.
-
Point-of-Care Ultrasound: A Multimodal Tool for the Management of Sepsis in the Emergency Department.Medicina (Kaunas). 2023 Jun 20;59(6):1180. doi: 10.3390/medicina59061180. Medicina (Kaunas). 2023. PMID: 37374384 Free PMC article. Review.
-
Sort and Sieve: Pre-Triage Screening of Patients with Suspected COVID-19 in the Emergency Department.Int J Environ Res Public Health. 2021 Sep 2;18(17):9271. doi: 10.3390/ijerph18179271. Int J Environ Res Public Health. 2021. PMID: 34501861 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
References
-
- Woloshin S, Patel N, Kesselheim AS. False negative tests for SARS‐CoV‐2 infection ‐ challenges and implications. N Engl J Med. 2020;383(6):e38. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
