

Evidence for a Window of Enhanced Plasticity in the Human Motor Cortex Following Ischemic Stroke
- PMID: 33576318
- PMCID: PMC7610679
- DOI: 10.1177/1545968321992330
Evidence for a Window of Enhanced Plasticity in the Human Motor Cortex Following Ischemic Stroke
Abstract
Background: In preclinical models, behavioral training early after stroke produces larger gains compared with delayed training. The effects are thought to be mediated by increased and widespread reorganization of synaptic connections in the brain. It is viewed as a period of spontaneous biological recovery during which synaptic plasticity is increased.
Objective: To look for evidence of a similar change in synaptic plasticity in the human brain in the weeks and months after ischemic stroke.
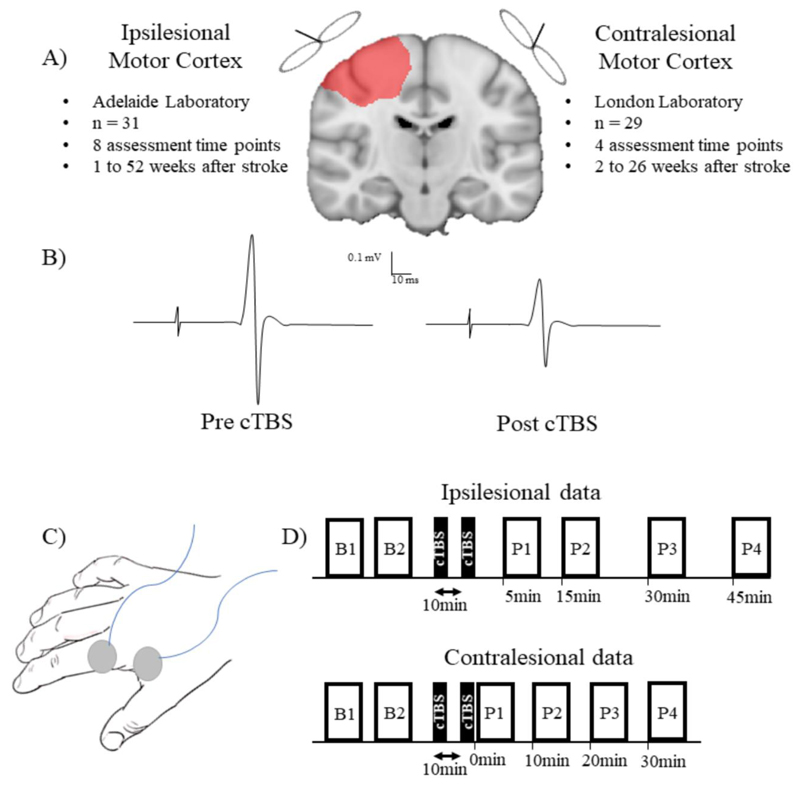
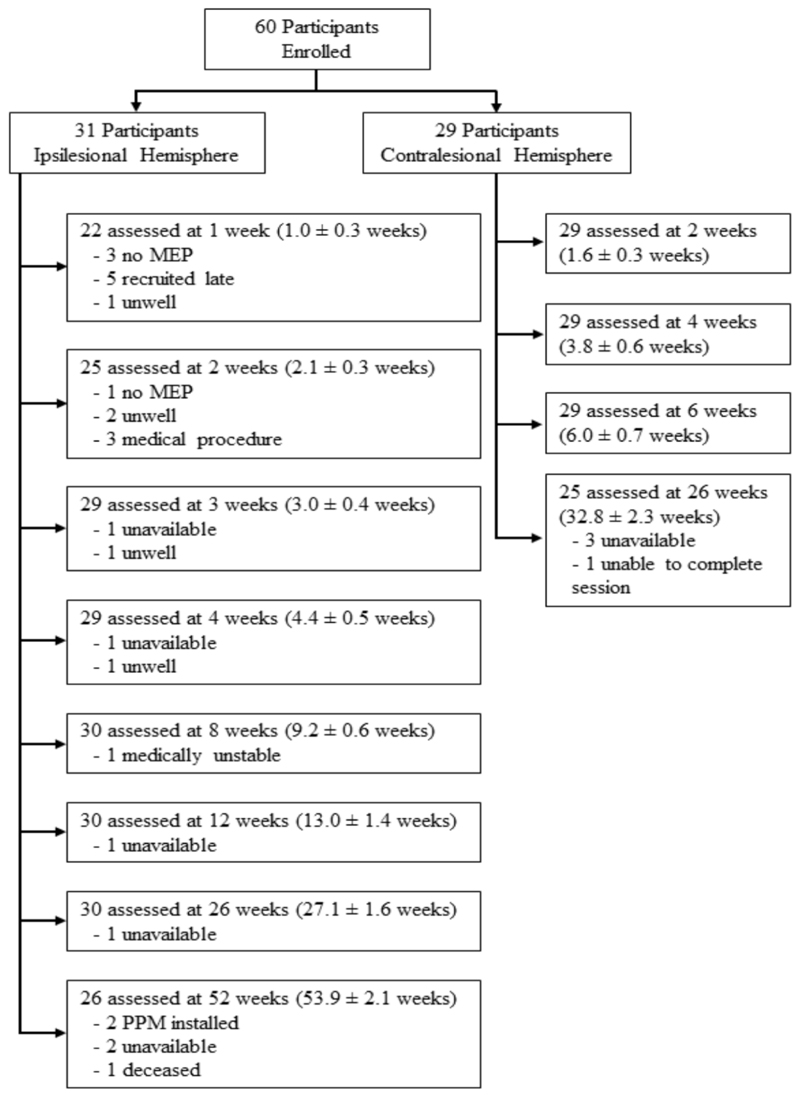
Methods: We used continuous theta burst stimulation (cTBS) to activate synapses repeatedly in the motor cortex. This initiates early stages of synaptic plasticity that temporarily reduces cortical excitability and motor-evoked potential amplitude. Thus, the greater the effect of cTBS on the motor-evoked potential, the greater the inferred level of synaptic plasticity. Data were collected from separate cohorts (Australia and UK). In each cohort, serial measurements were made in the weeks to months following stroke. Data were obtained for the ipsilesional motor cortex in 31 stroke survivors (Australia, 66.6 ± 17.8 years) over 12 months and the contralesional motor cortex in 29 stroke survivors (UK, 68.2 ± 9.8 years) over 6 months.
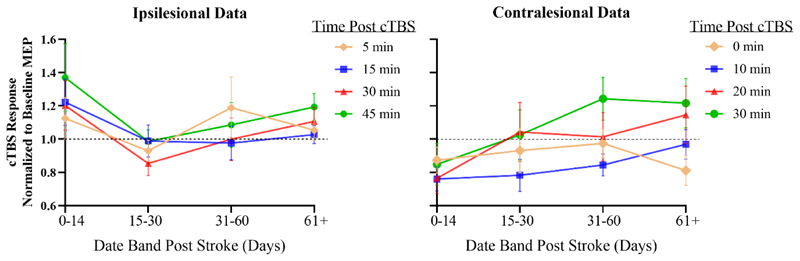
Results: Depression of cortical excitability by cTBS was most prominent shortly after stroke in the contralesional hemisphere and diminished over subsequent sessions (P = .030). cTBS response did not differ across the 12-month follow-up period in the ipsilesional hemisphere (P = .903).
Conclusions: Our results provide the first neurophysiological evidence consistent with a period of enhanced synaptic plasticity in the human brain after stroke. Behavioral training given during this period may be especially effective in supporting poststroke recovery.
Keywords: motor cortex; noninvasive brain stimulation; plasticity; recovery; stroke; transcranial magnetic stimulation.
Conflict of interest statement
None of the authors have potential conflicts of interest to be disclosed
Figures
References
-
- Prabhakaran S, Zarahn E, Riley C, et al. Inter-individual variability in the capacity for motor recovery after ischemic stroke. Neurorehabil Neural Repair. 2008;22:64–71. - PubMed
-
- Jorgensen HS, Nakayama H, Raaschou HO, Olsen TS. Stroke. Neurologic and functional recovery the Copenhagen Stroke Study. Phys Med Rehabil Clin N Am. 1999;10:887–906. - PubMed
-
- Hankey GJ, Spiesser J, Hakimi Z, et al. Rate, degree, and predictors of recovery from disability following ischemic stroke. Neurology. 2007;68:1583–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
