

Quantifying the gender gap in the HIV care cascade in southern Mozambique: We are missing the men
- PMID: 33577559
- PMCID: PMC7880488
- DOI: 10.1371/journal.pone.0245461
Quantifying the gender gap in the HIV care cascade in southern Mozambique: We are missing the men
Abstract
Background: HIV-infected men have higher rates of delayed diagnosis, reduced antiretroviral treatment (ART) retention and mortality than women. We aimed to assess, by gender, the first two UNAIDS 90 targets in rural southern Mozambique.
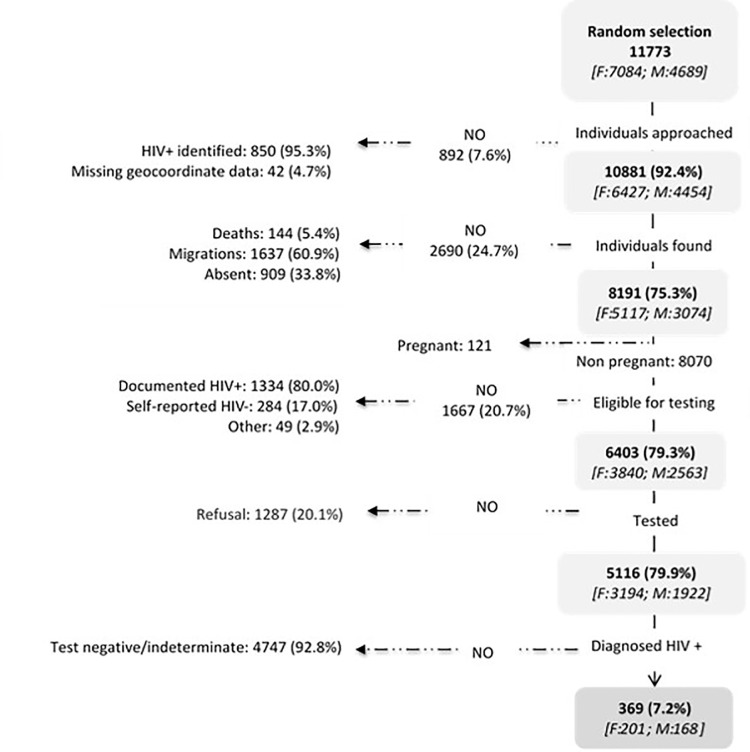
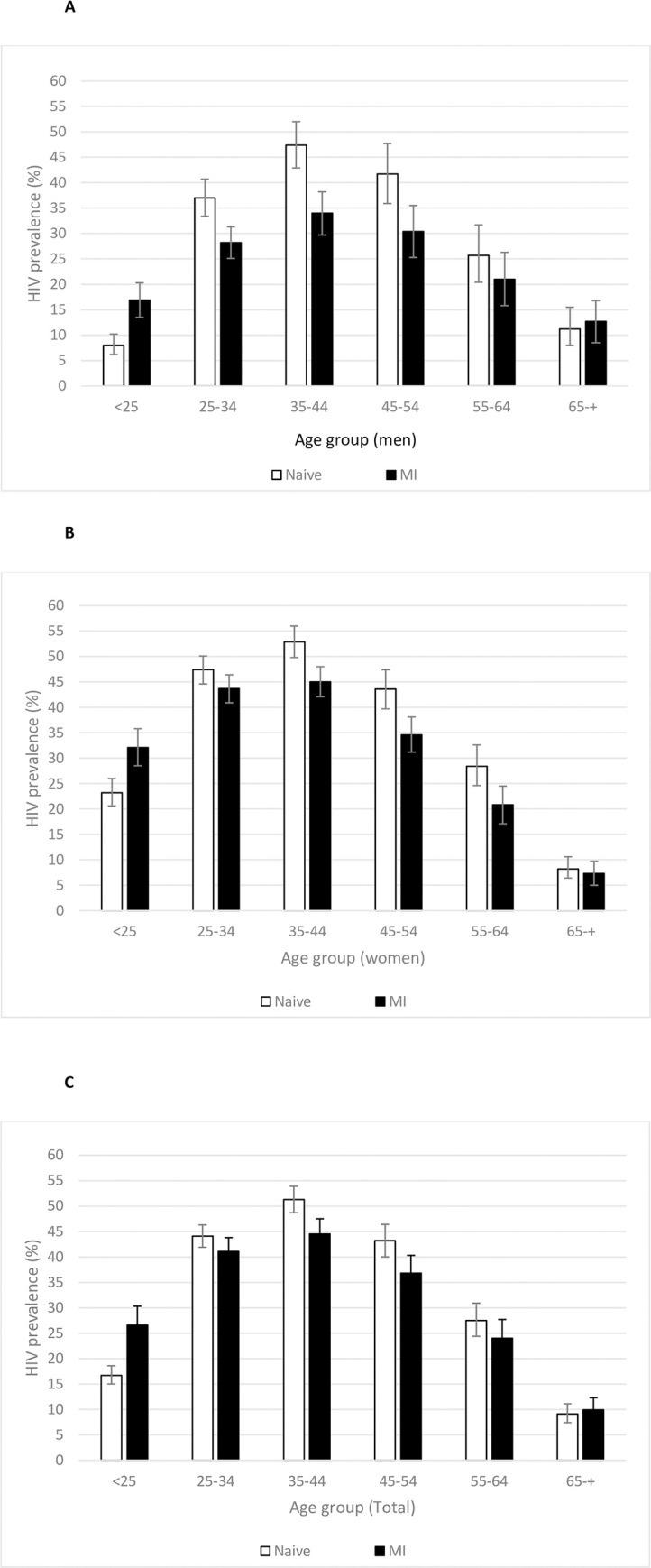
Methods: This analysis was embedded in a larger prospective cohort enrolling individuals with new HIV diagnosis between May 2014-June 2015 from clinic and home-based testing (HBT). We assessed gender differences between steps of the HIV-cascade. Adjusted HIV-community prevalence was estimated using multiple imputation (MI).
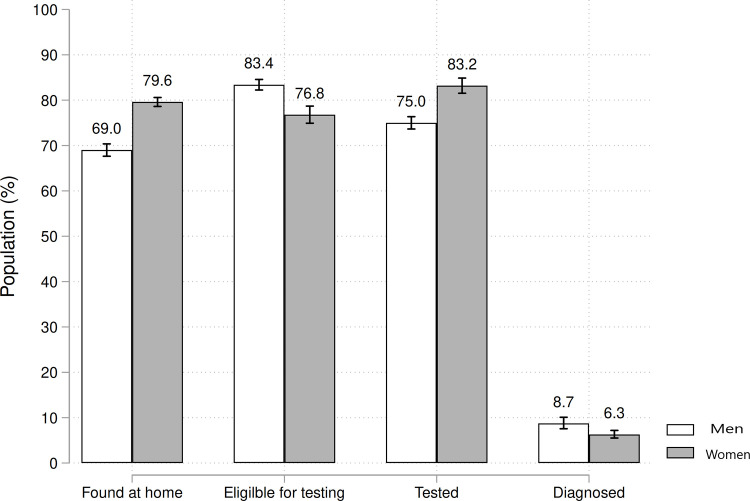
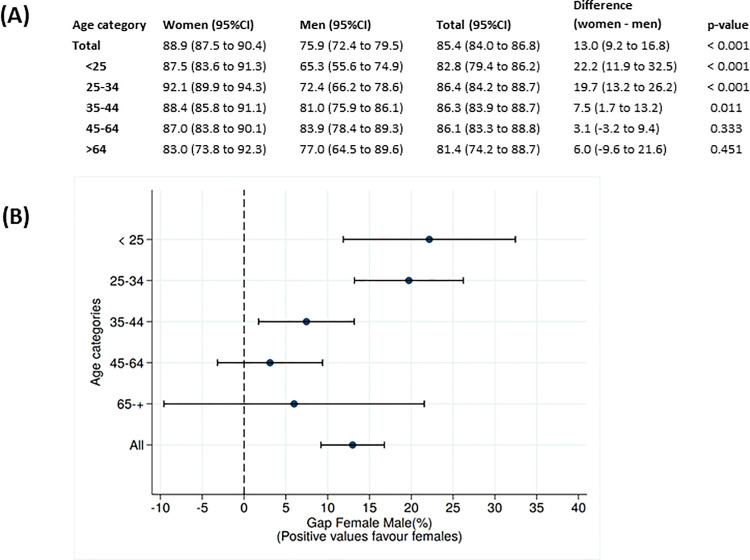
Results: Among 11,773 adults randomized in HBT (7084 female and 4689 male), the response rate before HIV testing was 48.7% among eligible men and 62.0% among women (p<0.001). MI did not significantly modify all-age HIV-prevalence for men but did decrease prevalence estimates in women from 36.4%to 33.0%. Estimated proportion of HIV-infected individuals aware of their status was 75.9% for men and 88.9% for women. In individuals <25 years, we observed up to 22.2% disparity in awareness of serostatus between genders. Among individuals eligible for ART, similar proportions of men and women initiated treatment (81.2% and 85.9%, respectively). Fourfold more men than womenwere in WHO stage III/IV AIDS at first clinical visit. Once on ART, men had a twofold higher 18-month loss to follow-up rate than women.
Conclusion: The contribution of missing HIV-serostatus data differentially impacted indicators of HIV prevalence and of achievement of UNAIDS targets by age and gender and men were missing long before the second 90. Increased efforts to characterize missing men and their needs will and their needs will allow us to urgently address the barriers to men accessing care and ensure men are not left behind in the UNAIDS 90-90-90 targets achievement.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- UNAIDS. Joint United Nations Programme on HIV/AIDS (UNAIDS). UNAIDS DATA 2017. 2017. - PubMed
-
- AIDSinfo | UNAIDS. [cited 7 Oct 2020]. Available: https://aidsinfo.unaids.org/.
-
- Reniers G, Slaymaker E, Nakiyingi-Miiro J, Nyamukapa C, Crampin AC, Herbst K, et al. Mortality trends in the era of antiretroviral therapy: evidence from the Network for Analysing Longitudinal Population based HIV/AIDS data on Africa (ALPHA). AIDS. 2014;28 Suppl 4: S533–42. 10.1097/QAD.0000000000000496 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
