

Perineal Wound Closure Following Abdominoperineal Resection and Pelvic Exenteration for Cancer: A Systematic Review and Meta-Analysis
- PMID: 33578769
- PMCID: PMC7916499
- DOI: 10.3390/cancers13040721
Perineal Wound Closure Following Abdominoperineal Resection and Pelvic Exenteration for Cancer: A Systematic Review and Meta-Analysis
Abstract
Background: Abdominoperineal resection (APR) and pelvic exenteration (PE) for the treatment of cancer require extensive pelvic resection with a high rate of postoperative complications. The objective of this work was to systematically review and meta-analyze the effects of vertical rectus abdominis myocutaneous flap (VRAMf) and mesh closure on perineal morbidity following APR and PE (mainly for anal and rectal cancers).
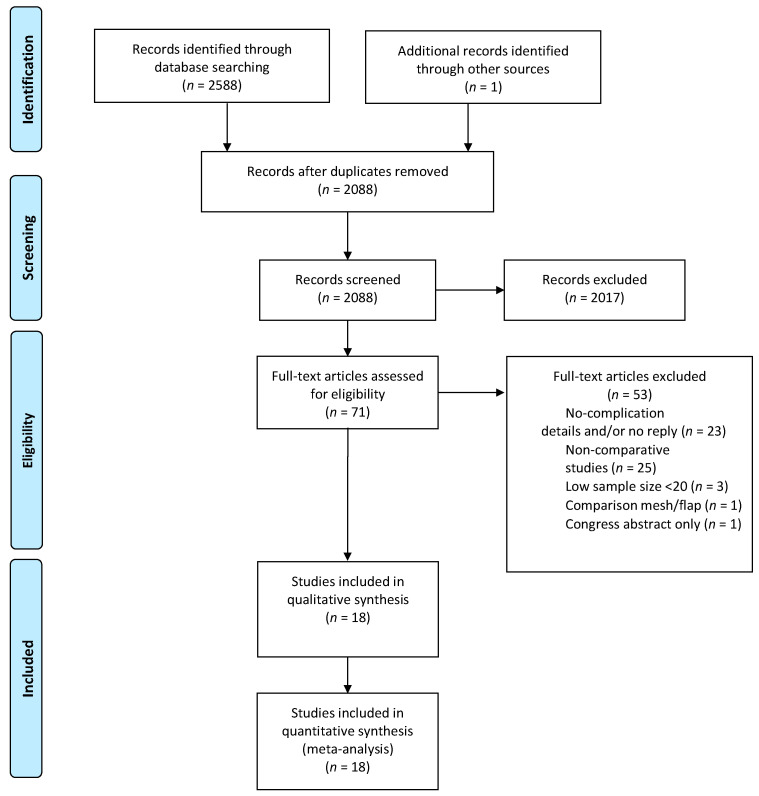
Methods: We searched PubMed, Cochrane, and EMBASE for eligible studies as of the year 2000. After data extraction, a meta-analysis was performed to compare perineal wound morbidity. The studies were distributed as follows: Group A comparing primary closure (PC) and VRAMf, Group B comparing PC and mesh closure, and Group C comparing PC and VRAMf in PE.
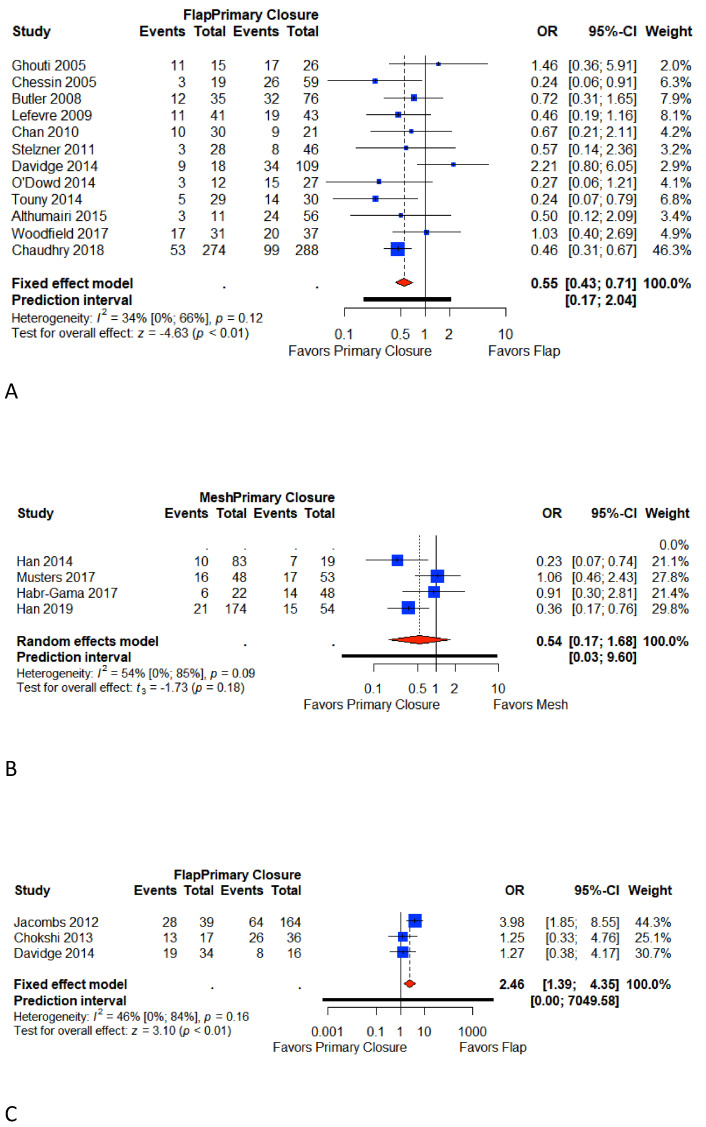
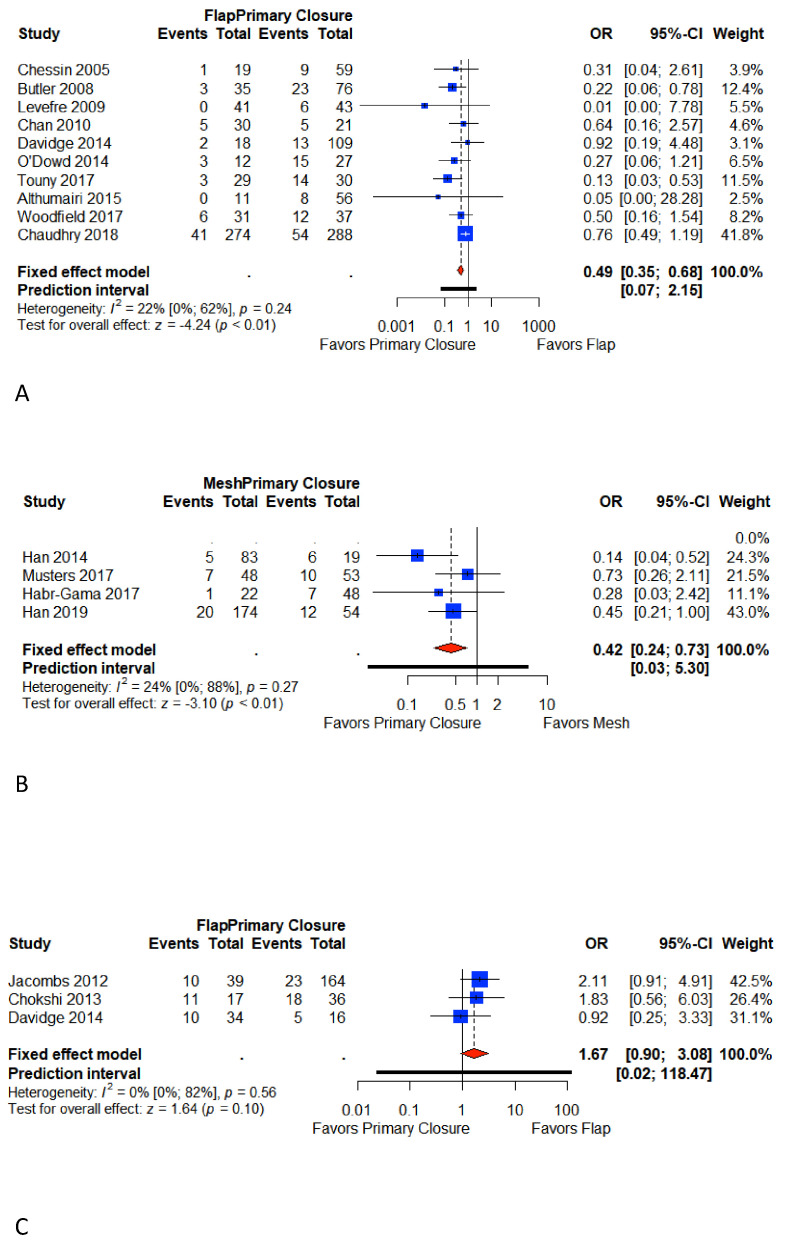
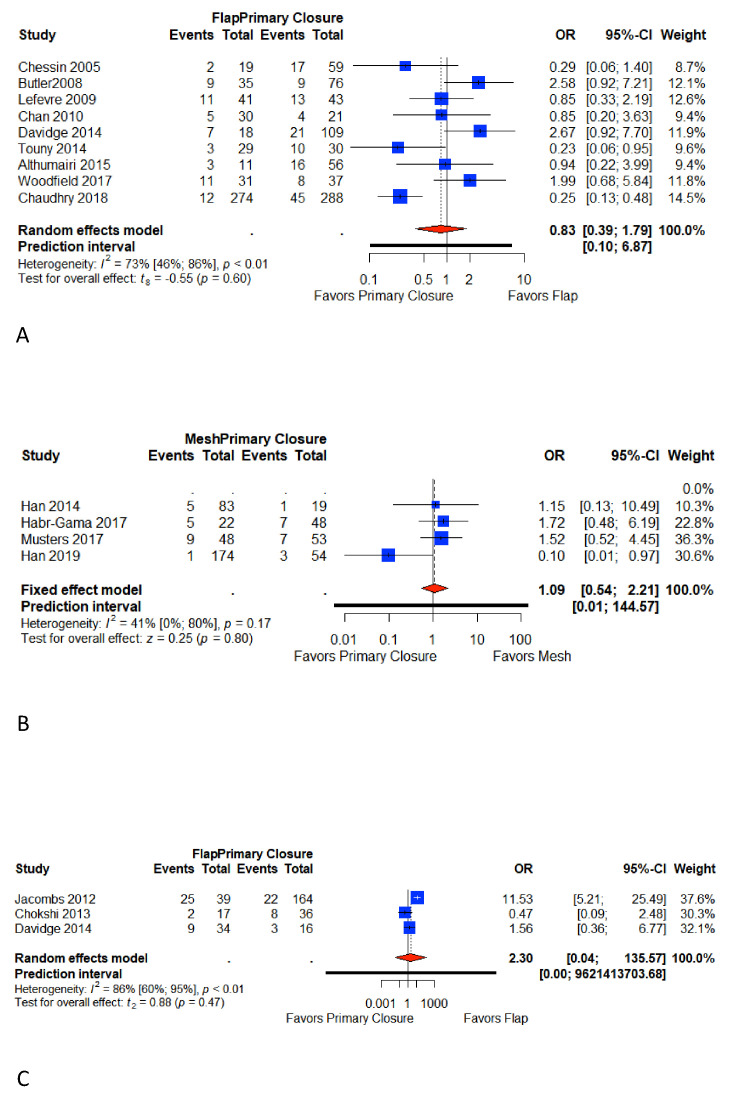
Results: Our systematic review yielded 18 eligible studies involving 2180 patients (1206 primary closures, 647 flap closures, 327 mesh closures). The meta-analysis of Groups A and B showed PC to be associated with an increase in the rate of total (Group A: OR 0.55, 95% CI 0.43-0.71; p < 0.01/Group B: OR 0.54, CI 0.17-1.68; p = 0.18) and major perineal wound complications (Group A: OR 0.49, 95% CI 0.35-0.68; p < 0.001/Group B: OR 0.38, 95% CI 0.12-1.17; p < 0.01). PC was associated with a decrease in total (OR 2.46, 95% CI 1.39-4.35; p < 0.01) and major (OR 1.67, 95% CI 0.90-3.08; p = 0.1) perineal complications in Group C.
Conclusion: Our results confirm the contribution of the VRAMf in reducing major complications in APR. Similarly, biological prostheses offer an interesting alternative in pelvic reconstruction. For PE, an adapted reconstruction must be proposed with specialized expertise.
Keywords: abdominoperineal resection; flap; mesh; perineal morbidity; perineal wound healing; rectal cancer; surgical oncology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Tuech J.-J., Pinson J., Nouhaud F.-X., Wood G., Clavier T., Sabourin J.-C., di Fiore F., Monge M., Papet E., Coget J. Total Pelvic Exenteration, Cytoreductive Surgery, and Hyperthermic Intraperitoneal Chemotherapy for Rectal Cancer with Associate Peritoneal Metastases: Surgical Strategies to Optimize Safety. Cancers. 2020;12:3478. doi: 10.3390/cancers12113478. - DOI - PMC - PubMed
-
- Denost Q., Solomon M., Tuech J.-J., Ghouti L., Cotte E., Panis Y., Lelong B., Rouanet P., Faucheron J.-L., Jafari M., et al. International variation in managing locally advanced or recurrent rectal cancer: Prospective benchmark analysis. BJS. 2020;107:1846–1854. doi: 10.1002/bjs.11854. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
