

Preoperative nutritional risk index and postoperative one-year skeletal muscle loss can predict the prognosis of patients with gastric adenocarcinoma: a registry-based study
- PMID: 33579228
- PMCID: PMC7881577
- DOI: 10.1186/s12885-021-07885-7
Preoperative nutritional risk index and postoperative one-year skeletal muscle loss can predict the prognosis of patients with gastric adenocarcinoma: a registry-based study
Abstract
Background: Patients with gastric cancer have an increased nutritional risk and experience a significant skeletal muscle loss after surgery. We aimed to determine whether muscle loss during the first postoperative year and preoperative nutritional status are indicators for predicting prognosis.
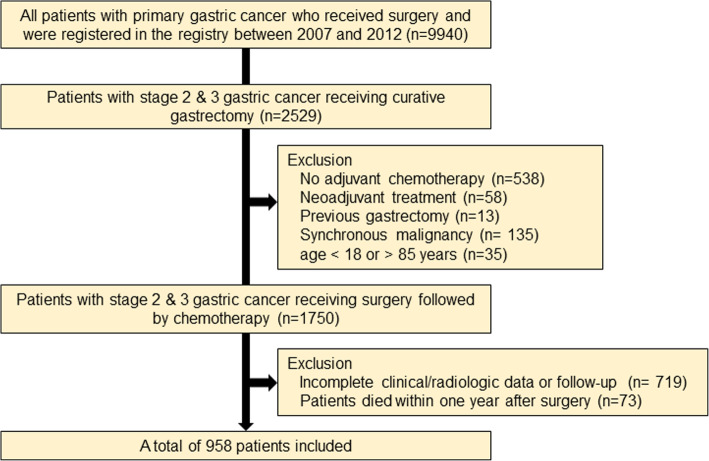
Methods: From a gastric cancer registry, a total of 958 patients who received curative gastrectomy followed by chemotherapy for stage 2 and 3 gastric cancer and survived longer than 1 year were investigated. Clinical and laboratory data were collected. Skeletal muscle index (SMI) was assessed based on the muscle area at the L3 level on abdominal computed tomography.
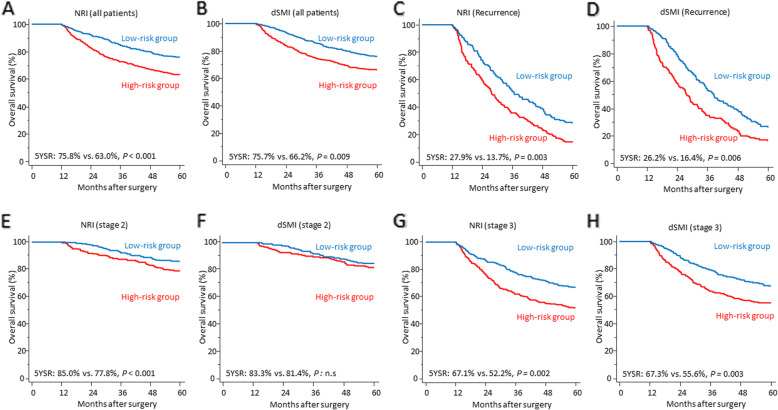
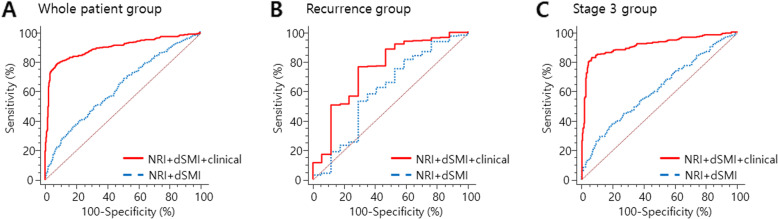
Results: Preoperative nutritional risk index (NRI) and postoperative decrement of SMI (dSMI) were significantly associated with overall survival (hazards ratio: 0.976 [95% CI: 0.962-0.991] and 1.060 [95% CI: 1.035-1.085], respectively) in a multivariate Cox regression analysis. Recurrence, tumor stage, comorbidity index were also significant prognostic indicators. Kaplan-Meier analyses exhibited that patients with higher NRI had a significantly longer survival than those with lower NRI (5-year overall survival: 75.8% vs. 63.0%, P < 0.001). In addition, a significantly better prognosis was observed in a patient group with less decrease of SMI (5-year overall survival: 75.7% vs. 66.2%, P = 0.009). A logistic regression analysis demonstrated that the performance of preoperative NRI and dSMI in mortality prediction was quite significant (AUC: 0.63, P < 0.001) and the combination of clinical factors enhanced the predictive accuracy to the AUC of 0.90 (P < 0.001). This prognostic relevance of NRI and dSMI was maintained in patients experiencing tumor recurrence and highlighted in those with stage 3 gastric adenocarcinoma.
Conclusions: Preoperative NRI is a predictor of overall survival in stage 2 or 3 gastric cancer patients and skeletal muscle loss during the first postoperative year was significantly associated with the prognosis regardless of relapse in stage 3 tumors. These factors could be valuable adjuncts for accurate prediction of prognosis in gastric cancer patients.
Keywords: Gastric cancer; Muscle loss; Nutrition; Prognosis; Sarcopenia; Surgery; Survival.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Braga M, Zuliani W, Foppa L, Di Carlo V, Cristallo M. Food intake and nutritional status after total gastrectomy: results of a nutritional follow-up. Br J Surg. 1988;75(5):477–480. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
