

Blood Parasite Load as an Early Marker to Predict Treatment Response in Visceral Leishmaniasis in Eastern Africa
- PMID: 33580234
- PMCID: PMC8423463
- DOI: 10.1093/cid/ciab124
Blood Parasite Load as an Early Marker to Predict Treatment Response in Visceral Leishmaniasis in Eastern Africa
Abstract
Background: To expedite the development of new oral treatment regimens for visceral leishmaniasis (VL), there is a need for early markers to evaluate treatment response and predict long-term outcomes.
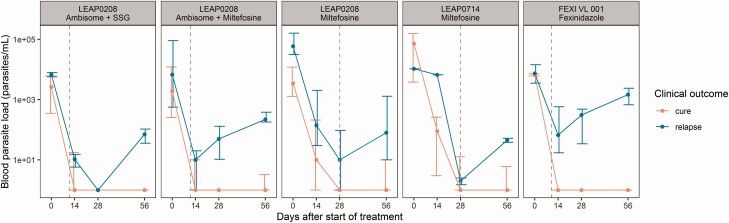
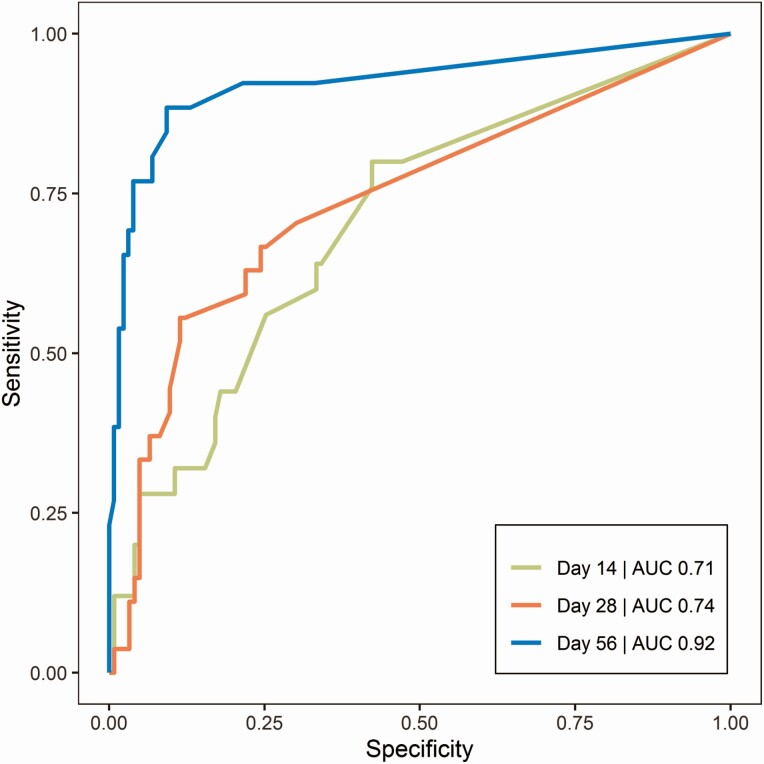
Methods: Data from 3 clinical trials were combined in this study, in which Eastern African VL patients received various antileishmanial therapies. Leishmania kinetoplast DNA was quantified in whole blood with real-time quantitative polymerase chain reaction (qPCR) before, during, and up to 6 months after treatment. The predictive performance of pharmacodynamic parameters for clinical relapse was evaluated using receiver-operating characteristic curves. Clinical trial simulations were performed to determine the power associated with the use of blood parasite load as a surrogate endpoint to predict clinical outcome at 6 months.
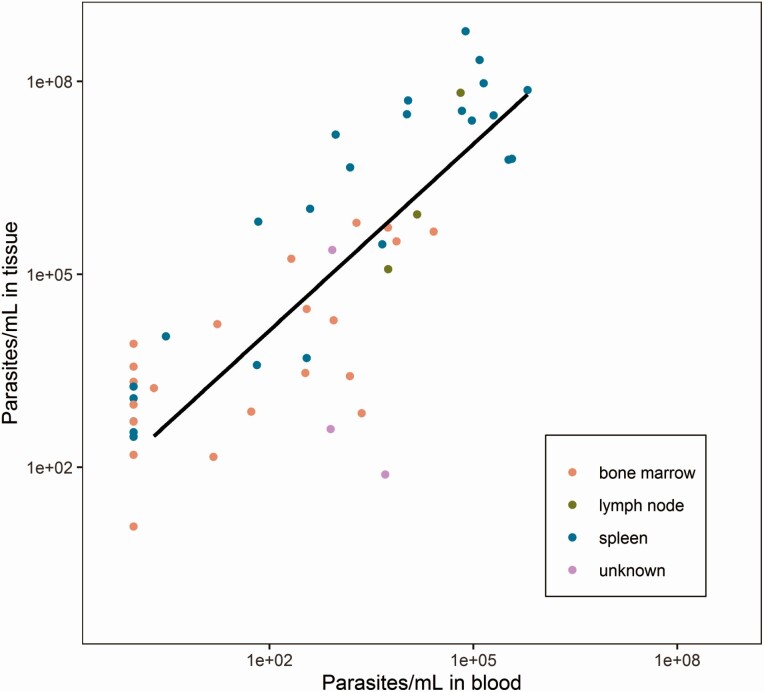
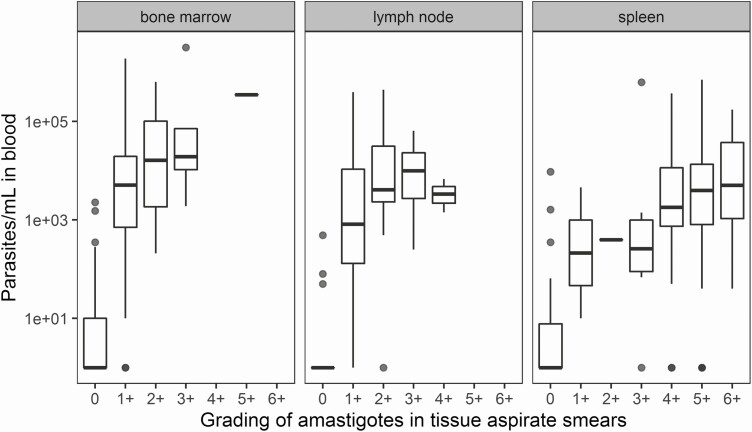
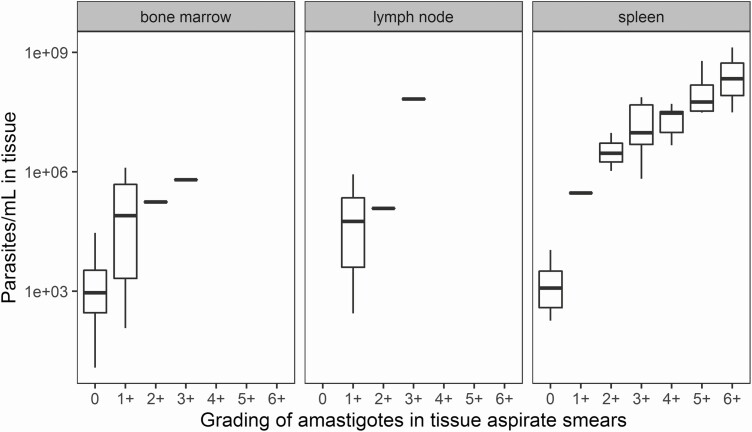
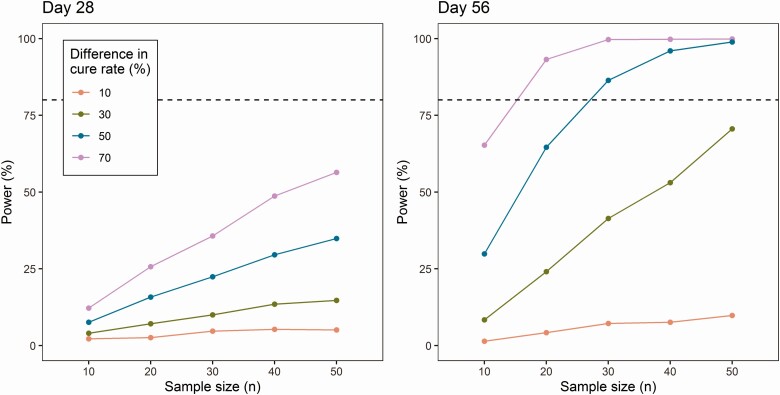
Results: The absolute parasite density on day 56 after start of treatment was found to be a highly sensitive predictor of relapse within 6 months of follow-up at a cutoff of 20 parasites/mL (area under the curve 0.92, specificity 0.91, sensitivity 0.89). Blood parasite loads correlated well with tissue parasite loads (ρ = 0.80) and with microscopy gradings of bone marrow and spleen aspirate smears. Clinical trial simulations indicated a > 80% power to detect a difference in cure rate between treatment regimens if this difference was high (> 50%) and when minimally 30 patients were included per regimen.
Conclusions: Blood Leishmania parasite load determined by qPCR is a promising early biomarker to predict relapse in VL patients. Once optimized, it might be useful in dose finding studies of new chemical entities.
Keywords: biomarker; parasitemia; pharmacodynamics; qPCR; visceral leishmaniasis.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- World Health Organization. Ending the neglect to attain the sustainable development goals—a road map for neglected tropical diseases 2021–2030. 2020:1–13. Available at: https://www.who.int/neglected_diseases/Revised-Draft-NTD-Roadmap-23Apr20.... Accessed 25 August 2020.
-
- World Health Organization. Control of the leishmaniases. Report of a meeting of the WHO expert committee on the control of leishmaniases, Geneva.2010: 49-51. Available at: https://apps.who.int/iris/bitstream/handle/10665/44412/WHO_TRS_949_eng.p.... Accessed 10 October 2020. - PubMed
-
- Rijal S, Ostyn B, Uranw S, et al. . Increasing failure of miltefosine in the treatment of Kala-azar in Nepal and the potential role of parasite drug resistance, reinfection, or noncompliance. Clin Infect Dis 2013; 56:1530–8. - PubMed
-
- Chulay JD, Bryceson AD. Quantitation of amastigotes of Leishmania donovani in smears of splenic aspirates from patients with visceral leishmaniasis. Am J Trop Med Hyg 1983; 32:475–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
