

Can Left Atrioventricular Valve Reduction Index (LAVRI) Predict the Surgical Strategy for Repair of Atrioventricular Septal Defect?
- PMID: 33580286
- PMCID: PMC8110484
- DOI: 10.1007/s00246-021-02558-5
Can Left Atrioventricular Valve Reduction Index (LAVRI) Predict the Surgical Strategy for Repair of Atrioventricular Septal Defect?
Abstract
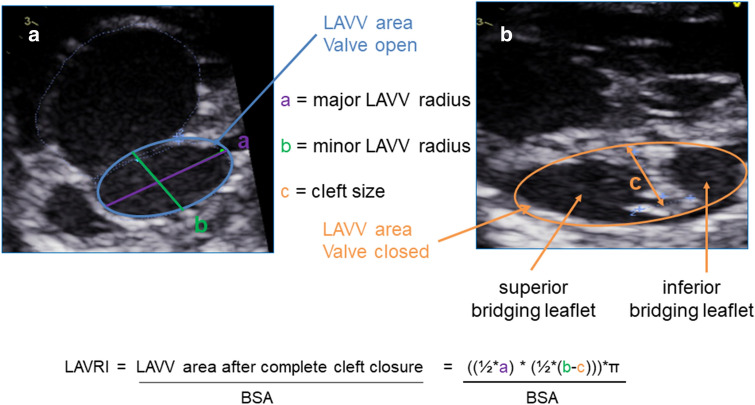
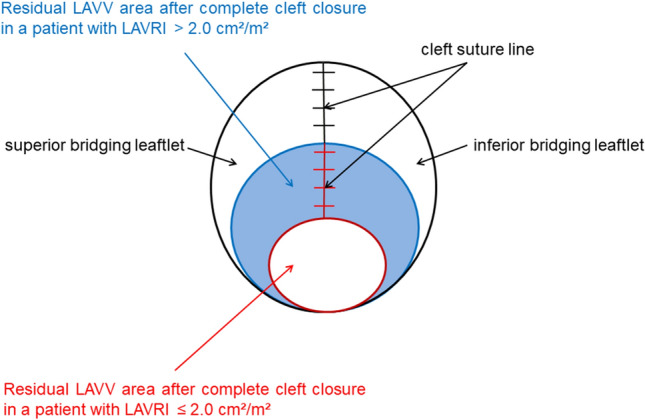
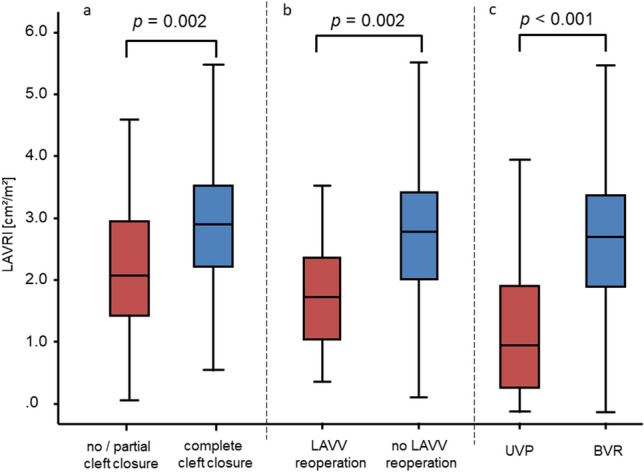
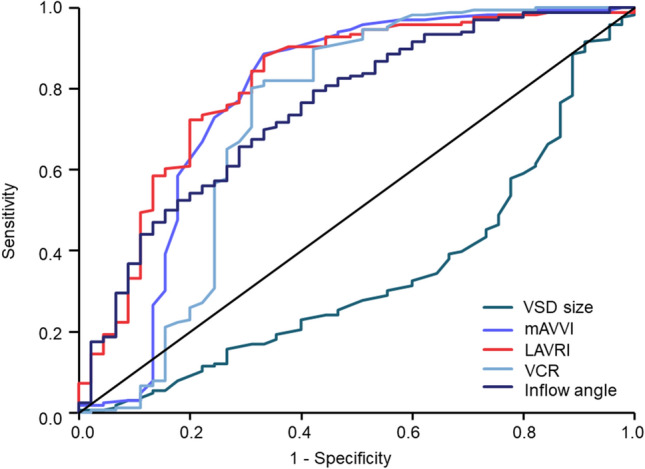
Despite improved survival, surgical treatment of atrioventricular septal defect (AVSD) remains challenging. The optimal technique for primary left atrioventricular valve (LAVV) repair and prediction of suitability for biventricular approach in unbalanced AVSD are still controversial. We evaluated the ability of our recently developed echocardiographic left atrioventricular valve reduction index (LAVRI) in predicting LAVV reoperation rate and surgical strategy for unbalanced AVSD. Retrospective echocardiographic analysis was available in 352 of 790 patients with AVSD treated in our institution and included modified atrioventricular valve index (mAVVI), ventricular cavity ratio (VCR), and right ventricle/left ventricle (RV/LV) inflow angle. LAVRI estimates LAVV area after complete cleft closure and was analyzed with regard to surgical strategy in primary LAVV repair and unbalanced AVSD. Of the entire cohort, 284/352 (80.68%) patients underwent biventricular repair and 68/352 (19.31%) patients underwent univentricular palliation. LAVV reoperation was performed in 25/284 (8.80%) patients after surgical correction of AVSD. LAVRI was significantly lower in patients requiring LAVV reoperation (1.92 cm2/m2 [IQR 1.31] vs. 2.89 cm2/m2 [IQR 1.37], p = 0.002) and significantly differed between patients receiving complete and no/partial cleft closure (2.89 cm2/m2 [IQR 1.35] vs. 2.07 cm2/m2 [IQR 1.69]; p = 0.002). Of 82 patients diagnosed with unbalanced AVSD, 14 were suitable for biventricular repair (17.07%). mAVVI, LAVRI, VCR, and RV/LV inflow angle accurately distinguished between balanced and unbalanced AVSD and predicted surgical strategy (all p < 0.001). LAVRI may predict surgical strategy in primary LAVV repair, LAVV reoperation risk, and suitability for biventricular approach in unbalanced AVSD anatomy.
Keywords: Atrioventricular septal defect; Echocardiographic analysis; Left atrioventricular valve repair; Preoperative decision-making; Unbalanced atrioventricular septal defect.
Conflict of interest statement
All authors declare not to have any conflicts of interest.
Figures
References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
