

The FAST-FURO study: effect of very early administration of intravenous furosemide in the prehospital setting to patients with acute heart failure attending the emergency department
- PMID: 33580790
- PMCID: PMC8245147
- DOI: 10.1093/ehjacc/zuaa042
The FAST-FURO study: effect of very early administration of intravenous furosemide in the prehospital setting to patients with acute heart failure attending the emergency department
Abstract
Aims: The effect of early administration of intravenous (IV) furosemide in the emergency department (ED) on short-term outcomes of acute heart failure (AHF) patients remains controversial, with one recent Japanese study reporting a decrease of in-hospital mortality and one Korean study reporting a lack of clinical benefit. Both studies excluded patients receiving prehospital IV furosemide and only included patients requiring hospitalization. To assess the impact on short-term outcomes of early IV furosemide administration by emergency medical services (EMS) before patient arrival to the ED.
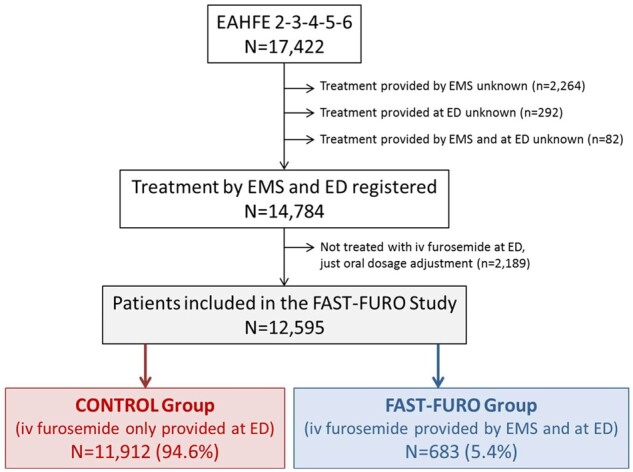
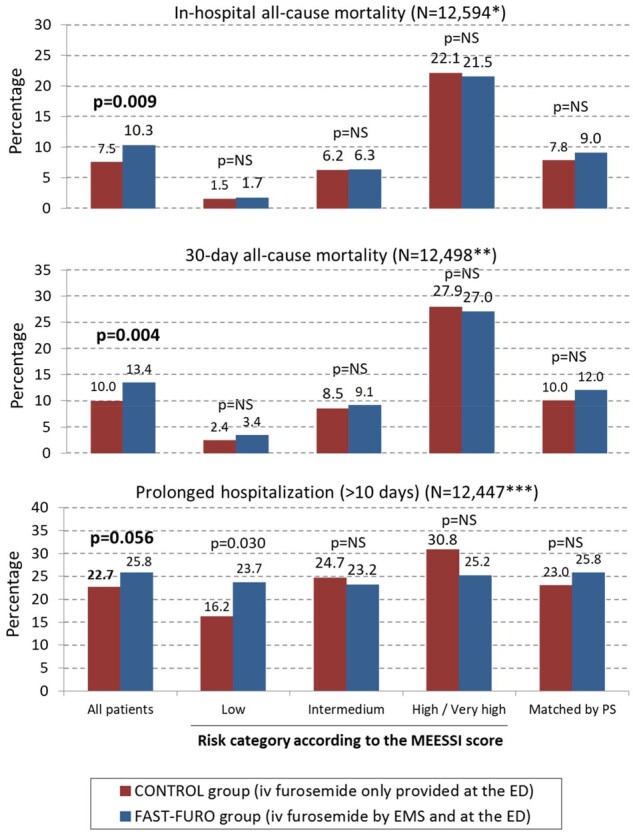
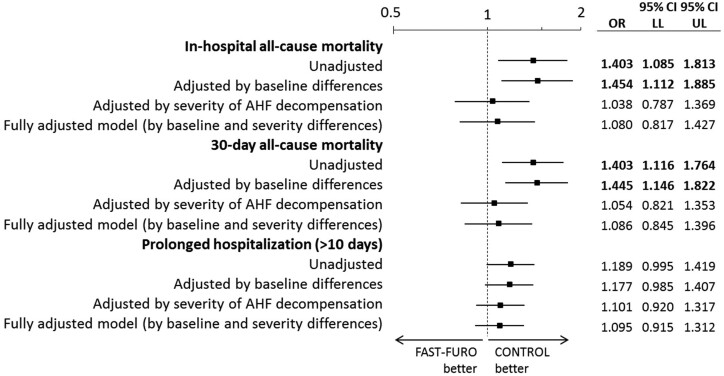
Methods and results: In a secondary analysis of the Epidemiology of Acute Heart Failure in Emergency Departments (EAHFE) registry of consecutive AHF patients admitted to Spanish EDs, patients treated with IV furosemide at the ED were classified according to whether they received IV furosemide from the EMS (FAST-FURO group) or not (CONTROL group). In-hospital all-cause mortality, 30-day all-cause mortality, and prolonged hospitalization (>10 days) were assessed. We included 12 595 patients (FAST-FURO = 683; CONTROL = 11 912): 968 died during index hospitalization [7.7%; FAST-FURO = 10.3% vs. CONTROL = 7.5%; odds ratio (OR) = 1.403, 95% confidence interval (95% CI) = 1.085-1.813; P = 0.009], 1269 died during the first 30 days (10.2%; FAST-FURO = 13.4% vs. CONTROL = 9.9%; OR = 1.403, 95% CI = 1.146-1.764; P = 0.004), and 2844 had prolonged hospitalization (22.8%; FAST-FURO = 25.8% vs. CONTROL = 22.6%; OR = 1.189, 95% CI = 0.995-1.419; P = 0.056). FAST-FURO group patients had more diabetes mellitus, ischaemic cardiomyopathy, peripheral artery disease, left ventricular systolic dysfunction, and severe decompensations, and had a better New York Heart Association class and had less atrial fibrillation. After adjusting for these significant differences, early IV furosemide resulted in no impact on short-term outcomes: OR = 1.080 (95% CI = 0.817-1.427) for in-hospital mortality, OR = 1.086 (95% CI = 0.845-1.396) for 30-day mortality, and OR = 1.095 (95% CI = 0.915-1.312) for prolonged hospitalization. Several sensitivity analyses, including analysis of 599 pairs of patients matched by propensity score, showed consistent findings.
Conclusion: Early IV furosemide during the prehospital phase was administered to the sickest patients, was not associated with changes in short-term mortality or length of hospitalization after adjustment for several confounders.
Keywords: Acute heart failure; Diuretics; Emergency department; Furosemide; Mortality; Outcome.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2021. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- -Chioncel O, Mebazaa A, Maggioni AP, Harjola VP, Rosano G, Laroche C, Piepoli MF, Crespo-Leiro MG, Lainscak M, Ponikowski P, Filippatos G, Ruschitzka F, Seferovic P, Coats AJS, Lund LH; ESC-EORP-HFA Heart Failure Long-Term Registry Investigators. Acute heart failure congestion and perfusion status—impact of the clinical classification on in-hospital and long-term outcomes; insights from the ESC-EORP-HFA Heart Failure Long-Term Registry. Eur J Heart Fail 2019;21:1338–1352. - PubMed
-
- -Javaloyes P, Miró Ò, Gil V, Martín‐Sánchez FJ, Jacob J, Herrero P, Takagi K, Alquézar‐Arbé A, López Díez MP, Martín E, Bibiano C, Escoda R, Gil C, Fuentes M, Llopis García G, Álvarez Pérez JM, Jerez A, Tost J, Llauger L, Romero R, Garrido JM, Rodríguez‐Adrada E, Sánchez C, Rossello X, Parissis J, Mebazaa A, Chioncel O, Llorens P; ICA-SEMES Research Group. Clinical phenotypes of acute heart failure based on signs and symptoms of perfusion and congestion at emergency department presentation and their relationship with patient management and outcomes. Eur J Heart Fail 2019;21:1353–1365. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola V-P, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P; Authors/Task Force Members. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016;37:2129–2200. - PubMed
-
- Llorens P, Miró Ò, Herrero P, Martín-Sánchez FJ, Jacob J, Valero A, Alonso H, Pérez-Durá MJ, Noval A, Gil-Román JJ, Zapater P, Llanos L, Gil V, Perelló R.. Clinical effects and safety of different strategies for administering intravenous diuretics in acutely decompensated heart failure: a randomised clinical trial. Emerg Med J 2014;31:706–713. - PubMed
-
- Ng KT, Yap JLL.. Continuous infusion vs. intermittent bolus injection of furosemide in acute decompensated heart failure: systematic review and meta-analysis of randomised controlled trials. Anaesthesia 2018;73:238–247. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
