

[Acute angle closure : An ophthalmological emergency in the emergency room]
- PMID: 33580819
- PMCID: PMC8897352
- DOI: 10.1007/s00063-021-00790-8
[Acute angle closure : An ophthalmological emergency in the emergency room]
Abstract
Background: The symptoms of acute angle closure, an emergency event that can lead to irreversible blindness without timely treatment, are diverse. Initially, these can be interpreted as internal or neurological diseases if headaches, pupil rigidity or nausea are in the foreground. The aim of our study was to assess the rate of harming and invasive diagnostics after primary presentation of patients with acute primary angle closure to nonophthalmologists.
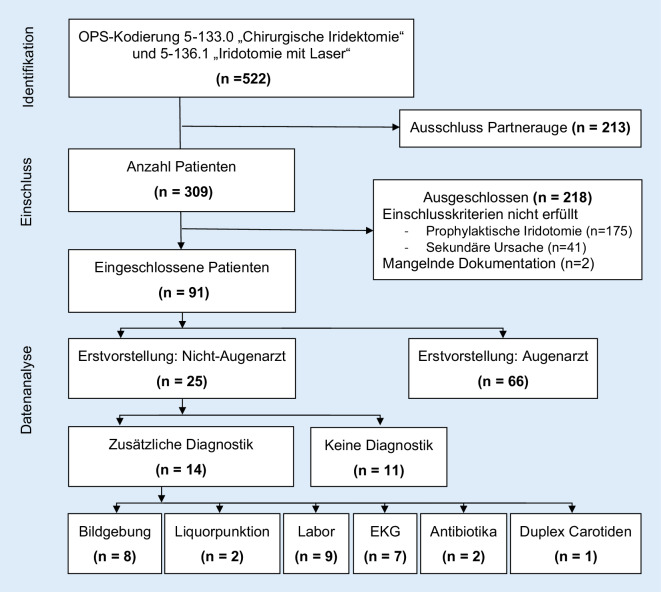
Methods: Retrospective single center study of patients with acute primary angle closure. To analyze these patients, all patients who were treated by surgical iridectomy (5-133.0) or iridotomy by laser (5-136.1) in the period 2014-2018 at the Eye Center at Medical Center, University of Freiburg (Germany), were identified. Subsequently, data analysis was carried out through file inspection to check the inclusion and exclusion criteria and the course of the disease.
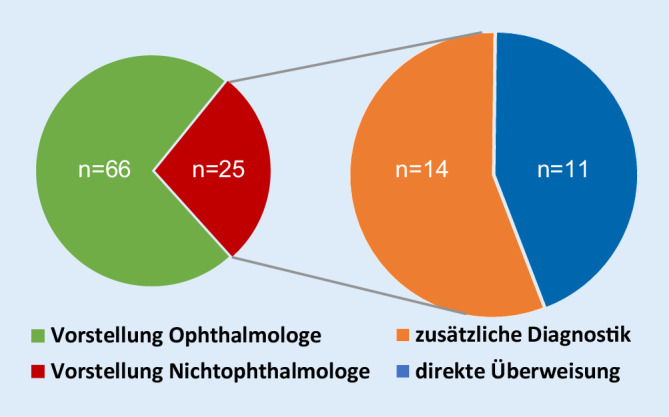
Results: In total, 91 patients with acute primary angle closure were included. Of these, 28% (n = 25) initially presented to nonophthalmological disciplines. In this patient group 56% (n = 11) received nontargeted diagnostics, with cranial imaging in 32% (n = 8) and lumbar puncture in 8% (n = 2).
Conclusion: Acute primary angle closure is associated with a high rate of nontargeted diagnostics by nonophthalmologists. Therefore, the clinical picture of acute angle closure should be in mind across all disciplines. With unspecific symptoms such as headaches, nausea and vomiting as well as pupil rigidity, the possibility of an acute increase in intraocular pressure caused by acute angle closure must be considered and early consultation with an ophthalmologist is recommended.
Zusammenfassung: HINTERGRUND: Die Symptome des akuten Winkelblocks, ein Notfallereignis, das ohne rechtzeitige Therapie zur irreversiblen Erblindung führen kann, sind vielfältig. Diese können initial als internistische oder neurologische Erkrankungen gedeutet werden, wenn Kopfschmerzen, Pupillenstarre oder Übelkeit im Vordergrund stehen. Ziel unserer Studie war es, die Rate belastender und invasiver Diagnostik durch primäre Vorstellung bei Nichtophthalmologen bei akutem primären Winkelblock zu erfassen.
Methode: Retrospektive Single-Center-Studie von Patienten mit akutem primärem Winkelblock. Zur Identifizierung dieser wurden alle Patienten erfasst, bei denen im Universitätsklinikum Freiburg, Klinik für Augenheilkunde im Zeitraum 2014–2018 eine chirurgische Iridektomie (5-133.0) oder Iridotomie durch Laser (5-136.1) durchgeführt wurde. Anschließend erfolgte durch Akteneinsicht die Datenanalyse zur Prüfung der Ein- und Ausschlusskriterien sowie des Krankheitsverlaufs.
Ergebnisse: Eingeschlossen wurden 91 Patienten mit akutem primären Winkelblock. Davon stellten sich 28 % (n = 25) initial bei nichtophthalmologischen Fachdisziplinen vor. In dieser Patientengruppe erhielten 56 % (n = 11) eine nichtzielführende Diagnostik, wobei bei 32 % (n = 8) eine kraniale Bildgebung und bei 8 % (n = 2) eine Lumbalpunktion durchgeführt wurde.
Schlussfolgerung: Bei akutem primären Winkelblock zeigt sich eine hohe Rate an nicht wegweisender Diagnostik durch Nichtophthalmologen, weshalb dieses Krankheitsbild fächerübergreifend präsent sein sollte. Bei unspezifischen Symptomen, wie Kopfschmerzen, Übelkeit und Erbrechen sowie Pupillenstarre, muss an die Möglichkeit eines akuten Augeninnendruckanstiegs durch einen akuten Winkelblock gedacht und das frühzeitige Hinzuziehen eines Ophthalmologen erwogen werden.
Keywords: Angle closure glaucoma; Diagnostic; Emergency room; Palpation; Symptom.
© 2021. The Author(s).


References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
