

Quality of Life After Bladder Cancer: A Cross-sectional Survey of Patient-reported Outcomes
- PMID: 33581875
- PMCID: PMC8082273
- DOI: 10.1016/j.eururo.2021.01.032
Quality of Life After Bladder Cancer: A Cross-sectional Survey of Patient-reported Outcomes
Abstract
Background: Little is known about health-related quality of life (HRQOL) following treatment for bladder cancer (BC).
Objective: To determine this, we undertook a cross-sectional survey covering 10% of the English population.
Design, setting, and participants: Participants 1-10 yr from diagnosis were identified through national cancer registration data.
Intervention: A postal survey was administered containing generic HRQOL and BC-specific outcome measures. Findings were compared with those of the general population and other pelvic cancer patients.
Outcome measurements and statistical analysis: Generic HRQOL was measured using five-level EQ-5D (EQ-5D-5L) and European Organization for Research and Treatment of Cancer quality of life questionnaire (EORTC QLQ)-C30. BC-specific outcomes were derived from EORTC QLQ-BLM30 and EORTC QLQ-NMIBC24.
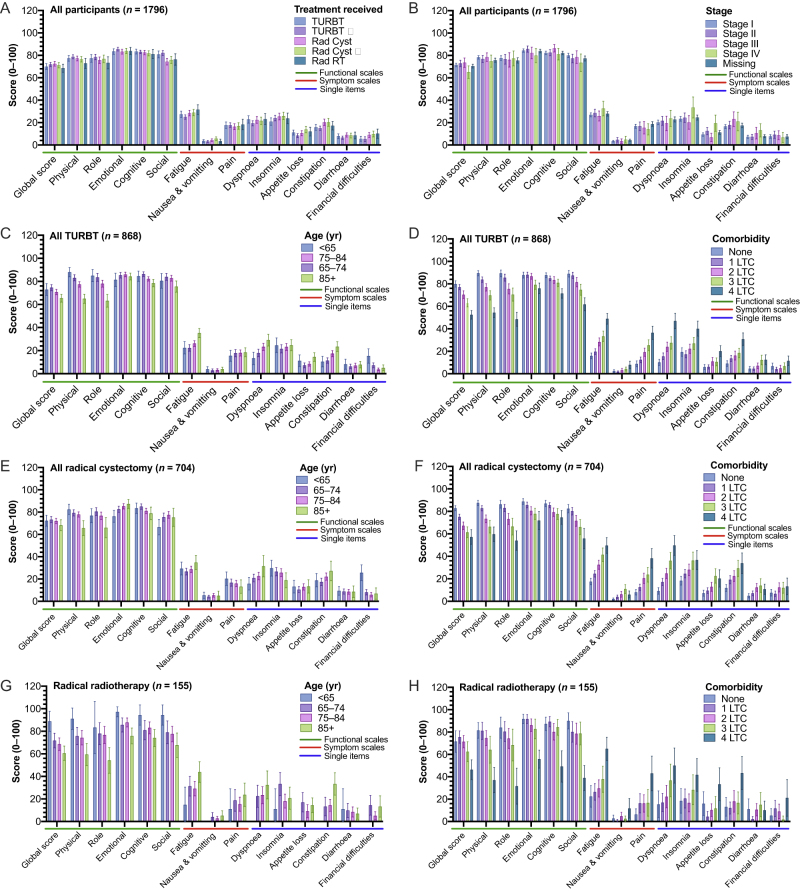
Results and limitations: A total of 1796 surveys were completed (response rate 55%), including 868 (48%) patients with non-muscle-invasive BC, 893 (50%) patients who received radiotherapy or radical cystectomy, and 35 (1.9%) patients for whom treatment was unknown. Most (69%) of the participants reported at least one problem in any EQ-5D dimension. Age/sex-adjusted generic HRQOL outcomes were similar across all stages and treatment groups, whilst problems increased with age (problems in one or more EQ-5D dimensions: <65 yr [67% {95% confidence interval or CI: 61-74}] vs 85+ yr [84% {95% CI: 81-89}], p = 0.016) and long-term conditions (no conditions [53% {95% CI: 48-58}] vs more than four conditions [94% {95% CI: 90-97}], p < 0.001). Sexual problems were reported commonly in men, increasing with younger age and radical treatment. Younger participants (under 65 yr) reported more financial difficulties (mean score 20 [95% CI: 16-25]) than those aged 85+ yr (6.8 [4.5-9.2], p < 0.001). HRQOL for BC patients (for comparison, males with problems in one or more EQ-5D dimensions 69% [95% CI: 66-72]) was significantly worse than what has been found after colorectal and prostate cancers and in the general population (51% [95% CI: 48-53], all p < 0.05).
Conclusions: HRQOL following BC appears to be relatively independent of disease stage, treatment, and multimodal care. Issues are reported with sexual function and financial toxicity. HRQOL after BC is worse than that after other pelvic cancers.
Patient summary: Patients living with bladder cancer often have reduced quality of life, which may be worse than that for other common pelvic cancer patients. Age and other illnesses appear to be more important in determining this quality of life than the treatments received. Many men complain of sexual problems. Younger patients have financial worries.
Keywords: Bacillus Calmette-Guerin; Bladder cancer; EQ-5D; Health-related quality of life; Patient-reported outcomes; Quality of life; Radical cystectomy.
Copyright © 2021 The Author(s). Published by Elsevier B.V. All rights reserved.
Figures


Comment in
-
Seeing the Unseen: Uncovering Patient-reported Outcomes in Bladder Cancer.Eur Urol. 2021 May;79(5):633-634. doi: 10.1016/j.eururo.2021.02.023. Epub 2021 Feb 23. Eur Urol. 2021. PMID: 33637365 No abstract available.
References
-
- Cumberbatch M.G.K., Jubber I., Black P.C. Epidemiology of bladder cancer: a systematic review and contemporary update of risk factors in 2018. Eur Urol. 2018;74:784–795. - PubMed
-
- Babjuk M., Burger M., Comperat E.M. European Association of Urology guidelines on non-muscle-invasive bladder cancer (TaT1 and carcinoma in situ)— 2019 update. Eur Urol. 2019;76:639–657. - PubMed
-
- Witjes J.A., Babjuk M., Bellmunt J. EAU-ESMO consensus statements on the management of advanced and variant bladder cancer—an international collaborative multistakeholder effort: under the auspices of the EAU-ESMO Guidelines Committees. Eur Urol. 2020;77:223–250. - PubMed
-
- Milowsky M.I., Rumble R.B., Booth C.M. Guideline on muscle-invasive and metastatic bladder cancer (European Association of Urology Guideline): American Society of Clinical Oncology clinical practice guideline endorsement. J Clin Oncol. 2016;34:1945–1952. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
