

Induced dysregulation of ACE2 by SARS-CoV-2 plays a key role in COVID-19 severity
- PMID: 33582450
- PMCID: PMC7862910
- DOI: 10.1016/j.biopha.2021.111363
Induced dysregulation of ACE2 by SARS-CoV-2 plays a key role in COVID-19 severity
Abstract
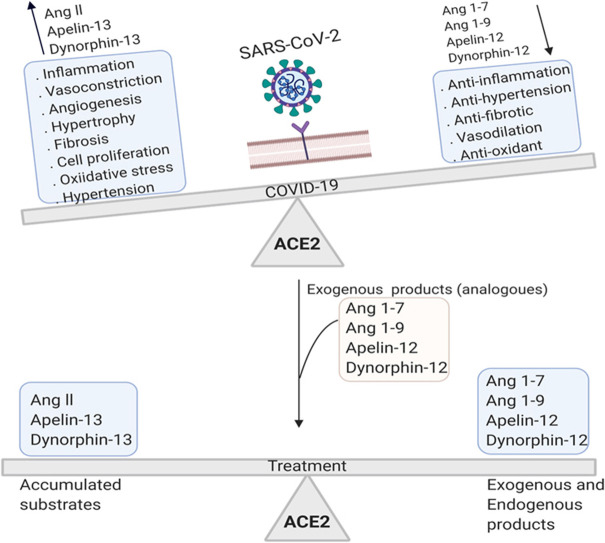
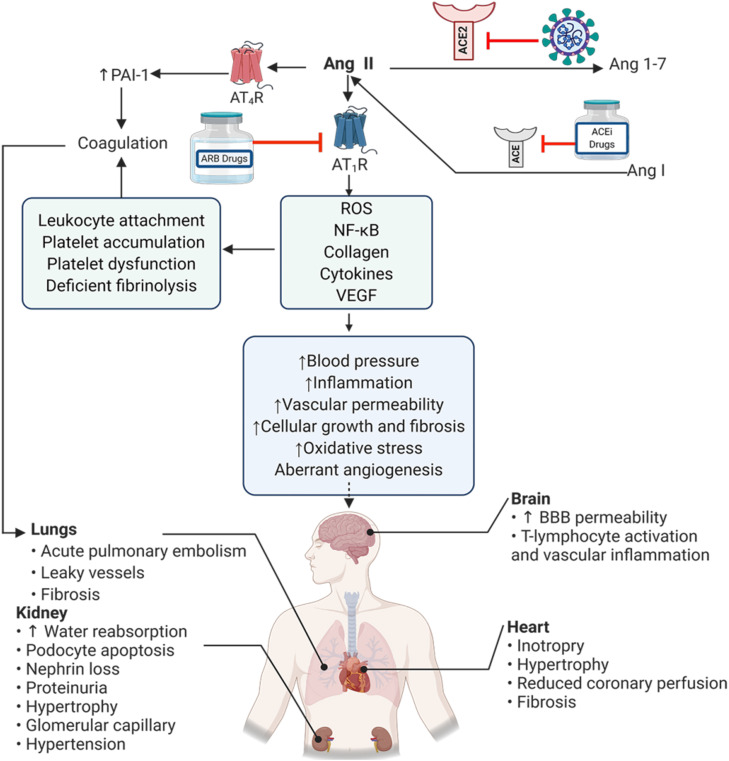
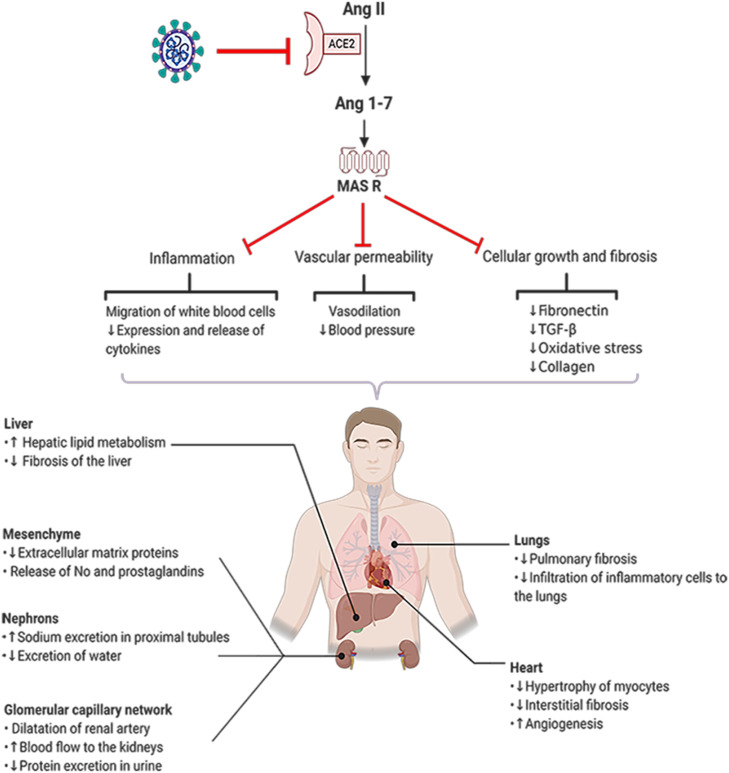
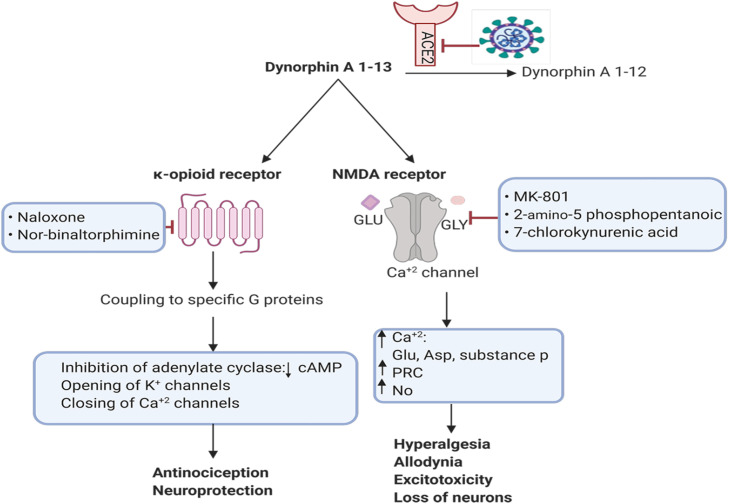
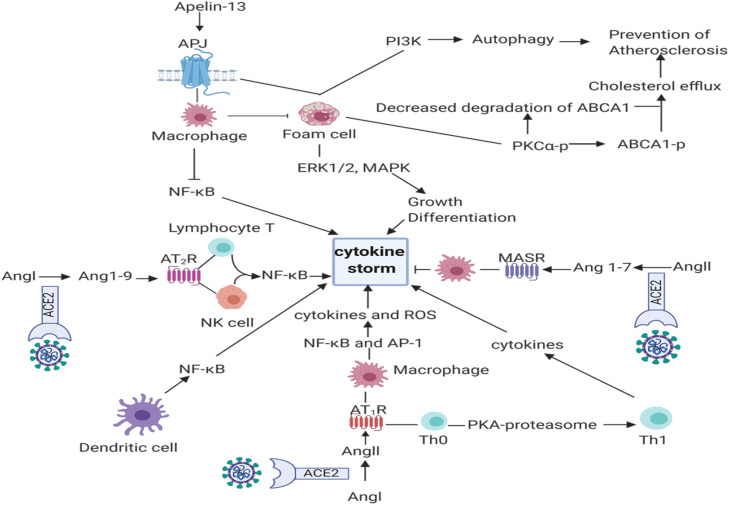
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), the cause of COVID-19, is reported to increase the rate of mortality worldwide. COVID-19 is associated with acute respiratory symptoms as well as blood coagulation in the vessels (thrombosis), heart attack and stroke. Given the requirement of angiotensin converting enzyme 2 (ACE2) receptor for SARS-CoV-2 entry into host cells, here we discuss how the downregulation of ACE2 in the COVID-19 patients and virus-induced shift in ACE2 catalytic equilibrium, change the concentrations of substrates such as angiotensin II, apelin-13, dynorphin-13, and products such as angiotensin (1-7), angiotensin (1-9), apelin-12, dynorphin-12 in the human body. Substrates accumulation ultimately induces inflammation, angiogenesis, thrombosis, neuronal and tissue damage while diminished products lead to the loss of the anti-inflammatory, anti-thrombotic and anti-angiogenic responses. In this review, we focus on the viral-induced imbalance between ACE2 substrates and products which exacerbates the severity of COVID-19. Considering the roadmap, we propose multiple therapeutic strategies aiming to rebalance the products of ACE2 and to ameliorate the symptoms of the disease.
Keywords: ACE2; Acute Respiratory Syndrome; Angiotensin; COVID-19; Cardiovascular Disease.
Copyright © 2021. Published by Elsevier Masson SAS.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Vickers C., Hales P., Kaushik V., Dick L., Gavin J., Tang J., Godbout K., Parsons T., Baronas E., Hsieh F. Hydrolysis of biological peptides by human angiotensin-converting enzyme-related carboxypeptidase. J. Biol. Chem. 2002;277(17):14838–14843. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
