

Endovascular Treatment of Ruptured Wide-Necked Anterior Communicating Artery Aneurysms Using a Low-Profile Visualized Intraluminal Support (LVIS) Device
- PMID: 33584512
- PMCID: PMC7876256
- DOI: 10.3389/fneur.2020.611875
Endovascular Treatment of Ruptured Wide-Necked Anterior Communicating Artery Aneurysms Using a Low-Profile Visualized Intraluminal Support (LVIS) Device
Abstract
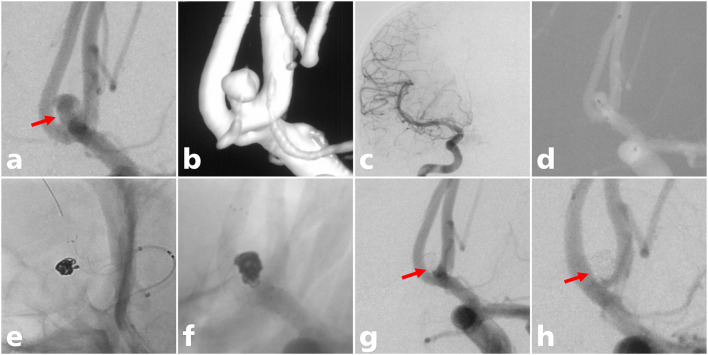
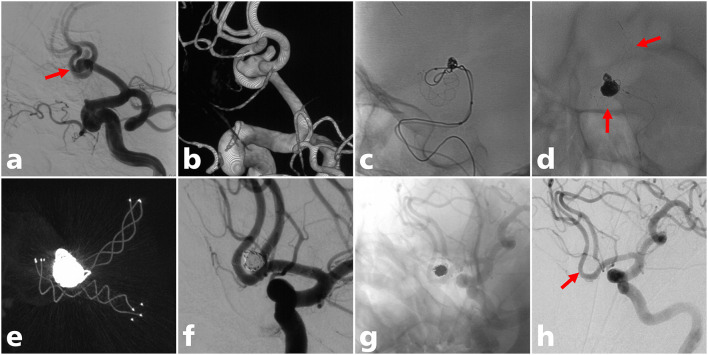
Objective: To evaluate the safety and efficacy of low-profile visualized intraluminal support (LVIS) stent-assisted coiling for the treatment of ruptured wide-necked anterior communicating artery (ACoA) aneurysms. Methods: The clinical and angiographic data of 31 acutely ruptured wide-necked ACoA aneurysms treated with LVIS stent-assisted coiling between January 2014 and December 2018 were retrospectively reviewed. Results: All stents were successfully deployed. The immediate angiographic results were modified Raymond-Roy class I in 27 cases, modified Raymond-Roy class II in 2 cases, and modified Raymond-Roy class IIIa in 2 cases. Intraoperative thrombosis and postoperative aneurysmal rebleeding occurred in one case each. Two patients (6.5%) who were admitted due to poor clinical grade conditions died during hospital admission as a result of initial bleeding. Angiographic follow-up (mean: 12.9 months) was performed for 26 patients, the results of which demonstrated that 25 aneurysms were completely occluded and one was class II. The last clinical follow-up (mean: 25.3 months) outcomes demonstrated that 27 patients had favorable clinical outcomes and two had poor clinical outcomes. Conclusion: LVIS stent-assisted coiling for ruptured wide-necked ACoA aneurysms was safe and effective, with a relatively low rate of perioperative complications and a high rate of complete occlusion at follow-up.
Keywords: LVIS stents; anterior communicating artery; intracranial aneurysm; ruptured; safety; wide-necked aneurysms.
Copyright © 2021 Xue, Liu, Xu, Fang, Li, Hong, Xu, Liu and Huang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Comparison of Low-Profiled Visualized Intraluminal Support Stent-Assisted Coiling and Coiling Only for Acutely Ruptured Intracranial Aneurysms: Safety and Efficacy Based on a Propensity Score-Matched Cohort Study.Neurosurgery. 2020 Sep 1;87(3):584-591. doi: 10.1093/neuros/nyaa110. Neurosurgery. 2020. PMID: 32415845
-
Treatment of wide-necked aneurysms with the Low-profile Visualized Intraluminal Support (LVIS Jr) device: a multicenter experience.J Neurointerv Surg. 2017 Nov;9(11):1098-1102. doi: 10.1136/neurintsurg-2016-012687. Epub 2016 Oct 27. J Neurointerv Surg. 2017. PMID: 27789790
-
Safety and efficacy of stent-assisted coiling for acutely ruptured wide-necked intracranial aneurysms: comparison of LVIS stents with laser-cut stents.Chin Neurosurg J. 2021 Mar 3;7(1):19. doi: 10.1186/s41016-021-00237-1. Chin Neurosurg J. 2021. PMID: 33653398 Free PMC article.
-
Utility of bulging technique for endovascular treatment of small and wide-necked aneurysms with a Low-profile Visualized Intraluminal Support (LVIS Jr.) device: A case report and review of the literature.Interv Neuroradiol. 2018 Apr;24(2):125-129. doi: 10.1177/1591019917743065. Epub 2017 Nov 21. Interv Neuroradiol. 2018. PMID: 29160136 Free PMC article. Review.
-
Efficacy and safety of PulseRider for treatment of wide-necked intracranial aneurysm-A systematic review and meta-analysis.Interv Neuroradiol. 2021 Feb;27(1):60-67. doi: 10.1177/1591019920940521. Epub 2020 Jul 7. Interv Neuroradiol. 2021. PMID: 32635777 Free PMC article.
Cited by
-
Independent predictors and risk score for intraprocedural rupture during endovascular treatment of small ruptured intracranial aneurysms (<5 mm).Front Neurol. 2022 Aug 24;13:923645. doi: 10.3389/fneur.2022.923645. eCollection 2022. Front Neurol. 2022. PMID: 36090846 Free PMC article.
-
Intra-procedural complications, success rate, and need for retreatment of endovascular treatments in anterior communicating artery aneurysms: a systematic review and meta-analysis.Neurosurg Rev. 2022 Oct;45(5):3157-3170. doi: 10.1007/s10143-022-01853-w. Epub 2022 Aug 27. Neurosurg Rev. 2022. PMID: 36029421
References
-
- Zheng Y, Zhou B, Wang X, Chen H, Fang X, Jiang P, et al. . Size, Aspect Ratio and Anatomic Location of Ruptured Intracranial Aneurysms: Consecutive Series of 415 Patients from a Prospective, Multicenter, Observational Study. Cell transplantation. (2019) 28:739–46. 10.1177/0963689718817227 - DOI - PMC - PubMed
-
- Beeckmans K, Crunelle CL, Van den Bossche J, Dierckx E, Michiels K, Vancoillie P, et al. . Cognitive outcome after surgical clipping versus endovascular coiling in patients with subarachnoid hemorrhage due to ruptured anterior communicating artery aneurysm. Acta neurologica Belgica. (2020) 120:123–32. 10.1007/s13760-019-01245-w - DOI - PubMed
-
- Molyneux AJ, Birks J, Clarke A, Sneade M, Kerr RS. The durability of endovascular coiling versus neurosurgical clipping of ruptured cerebral aneurysms: 18 year follow-up of the UK cohort of the International Subarachnoid Aneurysm Trial (ISAT). Lancet (London, England). (2015) 385:691–7. 10.1016/S0140-6736(14)60975-2 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources