

Case Report: Brain Metastasis Confined to the Infarcted Area Following Stroke
- PMID: 33584517
- PMCID: PMC7878549
- DOI: 10.3389/fneur.2020.617142
Case Report: Brain Metastasis Confined to the Infarcted Area Following Stroke
Abstract
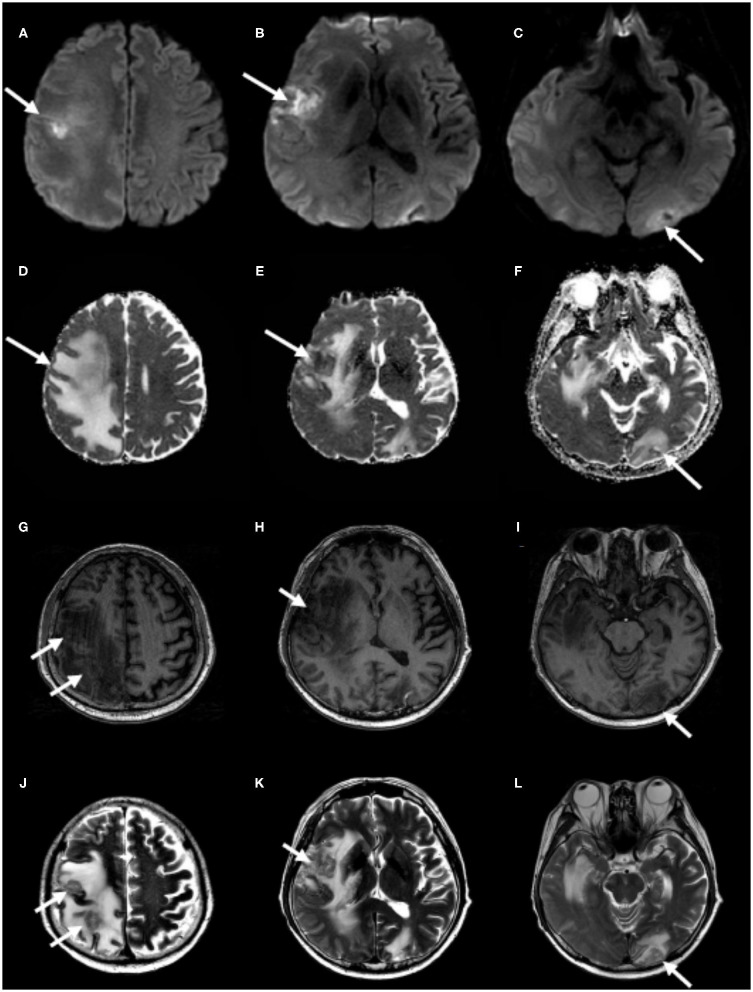
Background: Ischemic stroke and cancer are frequent in the elderly and are the two common causes of death and disability. They are related to each other, and cancer may lead to ischemic stroke and vice versa. If patients with cancer exhibited recurrent acute neurological deficits after index stroke, a cancer-related stroke could be considered. However, a brain metastasis is another common cause of neurological complications and has a poor prognosis in patients with ischemic stroke and comorbid cancer. Here, we report a rare case of metastatic cancer that occurred after index stroke in a patient with renal cell carcinoma (RCC) and unusual imaging findings. Through the case, we discuss the pathophysiology and probable predisposing factors for metastatic disease in areas of infarction. Case Presentation: A 48-year-old man presented with sudden onset of left facial palsy and hemiparesis. He had a history of hypertension and RCC with pulmonary metastases treated with radical nephrectomy and chemotherapy. Brain magnetic resonance imaging (MRI) revealed multiple scattered acute infarctions in the right insular, frontal, parietal, and left occipital cortices. There were no definite sources of embolism. Eight months after the index stroke, he presented with subacute onset of progressive left hemiparesis. He had no focal neurological deficits except left-sided weakness and left nasolabial fold blunting. MRI scan demonstrated partial diffusion restriction on the right frontotemporal cortices without decline of apparent diffusion coefficient values on the corresponding lesions and T1 hypointensities and T2 hyperintensities with perilesional vasogenic edema on the right insular, frontal, parietal, and left occipital cortices, indicative of brain metastases confined to the area of previous infarctions. Conclusions: Cerebral infarctions can cause neovascularization and disruption of the blood-brain barrier. Moreover, the compartmentalized cavity formed by the ischemic injury may accept a large volume of metastatic tumor cells. Such an altered microenvironment of infarcted tissue would be suitable for the colonization and proliferation of metastatic seed. Further, brain metastases should be considered, in addition to recurrence, when new focal neurological deficits develop in patients with ischemic stroke and comorbid cancer.
Keywords: cerebral infarction; magnetic resonance imaging; metastasis; neoplasm; renal cell carcinoma.
Copyright © 2021 Gwak, Hwang and Kim.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Brain metastasis localized to the same area of infarction: illustrative case.J Neurosurg Case Lessons. 2023 Aug 7;6(6):CASE23325. doi: 10.3171/CASE23325. Print 2023 Aug 7. J Neurosurg Case Lessons. 2023. PMID: 37581584 Free PMC article.
-
Sustained Opening of the Blood-Brain Barrier with Progressive Accumulation of White Matter Hyperintensities Following Ischemic Stroke.Brain Sci. 2019 Jan 21;9(1):16. doi: 10.3390/brainsci9010016. Brain Sci. 2019. PMID: 30669616 Free PMC article.
-
[Diffusion-weighted magnetic resonance imagings at the acute stage in two patients with spectacular shrinking deficit due to cardioembolic stroke].Rinsho Shinkeigaku. 2006 Feb;46(2):122-7. Rinsho Shinkeigaku. 2006. PMID: 16619836 Japanese.
-
[Brain tumor or stroke?].Ned Tijdschr Geneeskd. 2001 May 5;145(18):849-53. Ned Tijdschr Geneeskd. 2001. PMID: 11379393 Review. Dutch.
-
Cerebrovascular complications in cancer patients.Neurol Clin. 2003 Feb;21(1):167-92. doi: 10.1016/s0733-8619(02)00066-x. Neurol Clin. 2003. PMID: 12690649 Review.
Cited by
-
Brain metastasis localized to the same area of infarction: illustrative case.J Neurosurg Case Lessons. 2023 Aug 7;6(6):CASE23325. doi: 10.3171/CASE23325. Print 2023 Aug 7. J Neurosurg Case Lessons. 2023. PMID: 37581584 Free PMC article.
-
Predictive nomogram for ischemic stroke risk in clear cell renal cell carcinoma patients.Sci Rep. 2024 Dec 4;14(1):30162. doi: 10.1038/s41598-024-82072-9. Sci Rep. 2024. PMID: 39627344 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources