

Virtual Rehabilitation of the Paretic Hand and Arm in Persons With Stroke: Translation From Laboratory to Rehabilitation Centers and the Patient's Home
- PMID: 33584529
- PMCID: PMC7876436
- DOI: 10.3389/fneur.2021.623261
Virtual Rehabilitation of the Paretic Hand and Arm in Persons With Stroke: Translation From Laboratory to Rehabilitation Centers and the Patient's Home
Abstract
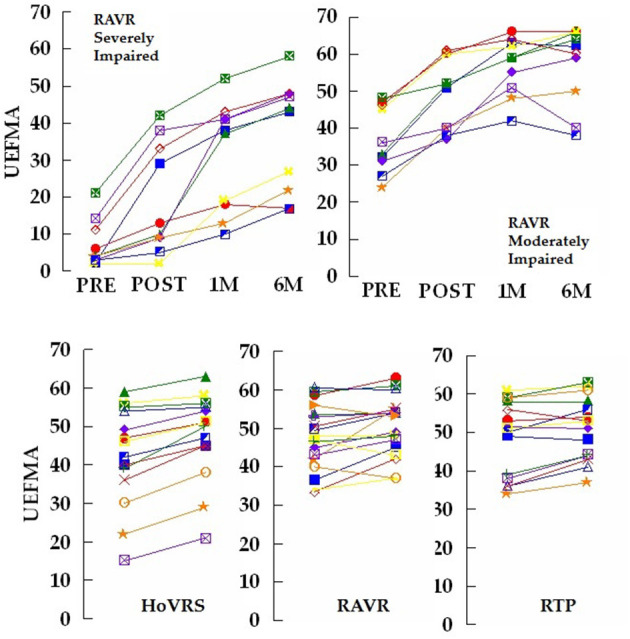
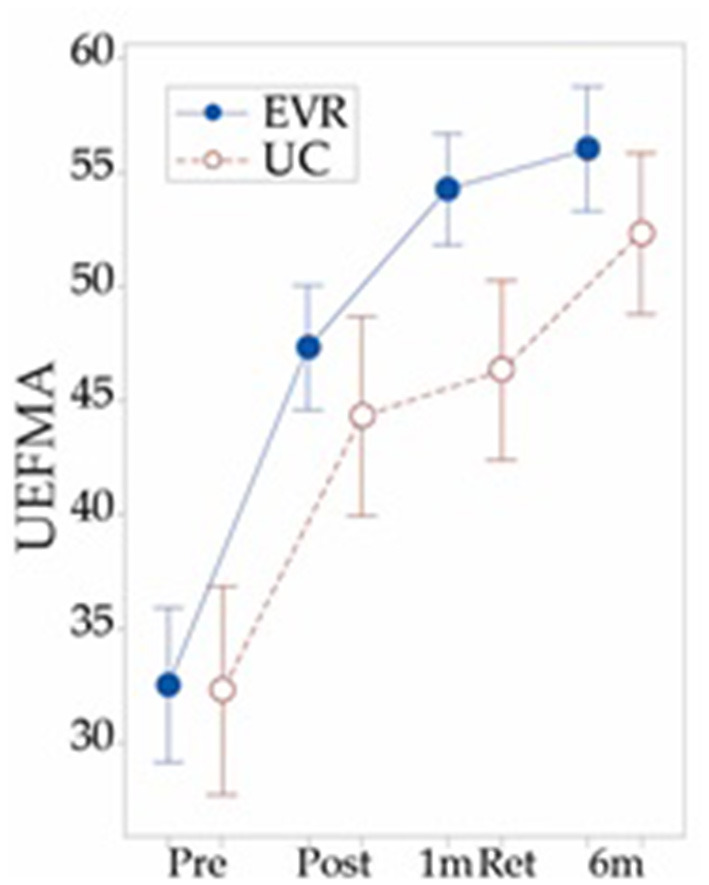
The anatomical and physiological heterogeneity of strokes and persons with stroke, along with the complexity of normal upper extremity movement make the possibility that any single treatment approach will become the definitive solution for all persons with upper extremity hemiparesis due to stroke unlikely. This situation and the non-inferiority level outcomes identified by many studies of virtual rehabilitation are considered by some to indicate that it is time to consider other treatment modalities. Our group, among others, has endeavored to build on the initial positive outcomes in studies of virtual rehabilitation by identifying patient populations, treatment settings and training schedules that will best leverage virtual rehabilitation's strengths. We feel that data generated by our lab and others suggest that (1) persons with stroke may adapt to virtual rehabilitation of hand function differently based on their level of impairment and stage of recovery and (2) that less expensive, more accessible home based equipment seems to be an effective alternative to clinic based treatment that justifies continued optimism and study.
Keywords: arm; hand; rehabilitation; stroke; virtual reality.
Copyright © 2021 Fluet, Qiu, Patel, Mont, Cronce, Yarossi, Merians and Adamovich.
Conflict of interest statement
GF, QQ, AMo, AC, AMe, and SA have applied for a patent for the Home Virtual Rehabilitation System. QQ, AMo, and AC have interests in NeuroTech3R, a company working toward bringing the Home Virtual Rehabilitation System to market. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- iBadia BS, Fluet GG, Llorens R, Deutsch JE. Virtual reality for sensorimotor rehabilitation post stroke: design principles and evidence. In: Reinkensmeyer D, Dietz V. editors. Neurorehabilitation Technology. Cham: Springer; (2016). p. 573–603. 10.1007/978-3-319-28603-7_28 - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous