

Total Elbow Arthroplasty in an Older Patient with a Forearm Amputation: A Case Report in a Spastic Elbow
- PMID: 33585312
- PMCID: PMC7857651
- DOI: 10.13107/jocr.2020.v10.i07.1906
Total Elbow Arthroplasty in an Older Patient with a Forearm Amputation: A Case Report in a Spastic Elbow
Abstract
Introduction: Total elbow arthroplasty is a common procedure in older patients after comminuted distal humerus fractures. However, in patients with a forearm amputation, this treatment indication is less obvious.
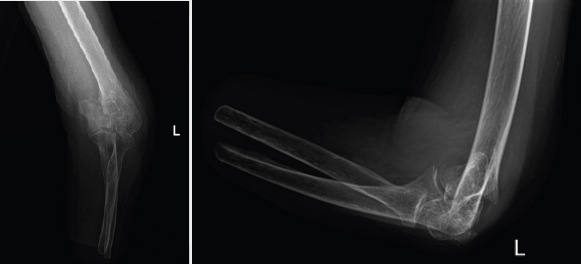
Case report: We report the case of an older spastic patient with bilateral forearm amputation for whom we performed a total elbow arthroplasty for a complex left distal humerus fracture. At 1 year follow-up, our patient was satisfied with the outcome as she had recovered her previous range motion and autonomy. There was no sign of implant loosening or migration on radiographs.
Conclusions: Given that this treatment has the same benefits as in the typical target population and that any complications that may occur could be less devastating in a patient with forearm amputation. We think that elbow arthroplasty should be offered, in case of complex articular fracture, to all older patients with forearm amputation who has functional demands.
Keywords: Elbow replacement arthroplasty; amputation; elderly; forearm; humeral fractures; spasticity.
Copyright: © Indian Orthopaedic Research Group.
Conflict of interest statement
Conflict of Interest: Nil
Figures



Similar articles
-
Distal humeral fractures treated with noncustom total elbow replacement.J Bone Joint Surg Am. 2004 May;86(5):940-7. doi: 10.2106/00004623-200405000-00009. J Bone Joint Surg Am. 2004. PMID: 15118036
-
Complex fractures of the distal humerus in the elderly: is primary total elbow arthroplasty a valid treatment alternative? A series of 20 cases.Orthop Traumatol Surg Res. 2013 Feb;99(1):10-20. doi: 10.1016/j.otsr.2012.10.010. Epub 2012 Dec 27. Orthop Traumatol Surg Res. 2013. PMID: 23273377
-
Long-term outcomes of total elbow arthroplasty for distal humeral fracture: results from a prior randomized clinical trial.J Shoulder Elbow Surg. 2019 Nov;28(11):2198-2204. doi: 10.1016/j.jse.2019.06.004. Epub 2019 Aug 21. J Shoulder Elbow Surg. 2019. PMID: 31445787
-
Total elbow arthroplasty for the treatment of insufficient distal humeral fractures. A retrospective clinical study and review of the literature.Injury. 2009 Jun;40(6):582-90. doi: 10.1016/j.injury.2009.01.123. Epub 2009 Apr 24. Injury. 2009. PMID: 19394013 Review.
-
Total elbow arthroplasty for distal humerus fractures.Orthop Clin North Am. 2013 Jul;44(3):381-7, ix-x. doi: 10.1016/j.ocl.2013.03.009. Epub 2013 May 4. Orthop Clin North Am. 2013. PMID: 23827840 Review.
References
-
- Robinson CM, Hill RM, Jacobs N, Dall G, Court-Brown CM. Adult distal humeral metaphyseal fractures: epidemiology and results of treatment. J Orthop Trauma. 2003;17:38–47. - PubMed
-
- Bonnevialle P, Ferron JM. Les fractures des sujets âgés de plus de 80 ans. Rev Chir Orthop. 2003;89(Suppl. 5):S129–82.
-
- John H, Rosso R, Neff U, Bodoky A, Regazzoni P, Harder F. Operative treatment of distal humeral fractures in the elderly. J Bone Joint Surg Br. 1994;76:793–6. - PubMed
-
- Lecestre P, Aubanial JM, Claisse PR. Severe fractures of the lower end of the humerus in adults (author's translation) Rev Chir Orthop. 1980;66(Suppl. 2):20–50.
-
- Pereles TR, Koval KJ, Gallagher M, Rosen H. Open reduction and internal fixation of the distal humerus:functional outcome in the elderly. J Trauma. 1997;43:578–84. - PubMed
Publication types
LinkOut - more resources
Full Text Sources