

Validation of the Role of Thrombin Generation Potential by a Fully Automated System in the Identification of Breast Cancer Patients at High Risk of Disease Recurrence
- PMID: 33585786
- PMCID: PMC7875677
- DOI: 10.1055/s-0040-1722609
Validation of the Role of Thrombin Generation Potential by a Fully Automated System in the Identification of Breast Cancer Patients at High Risk of Disease Recurrence
Abstract
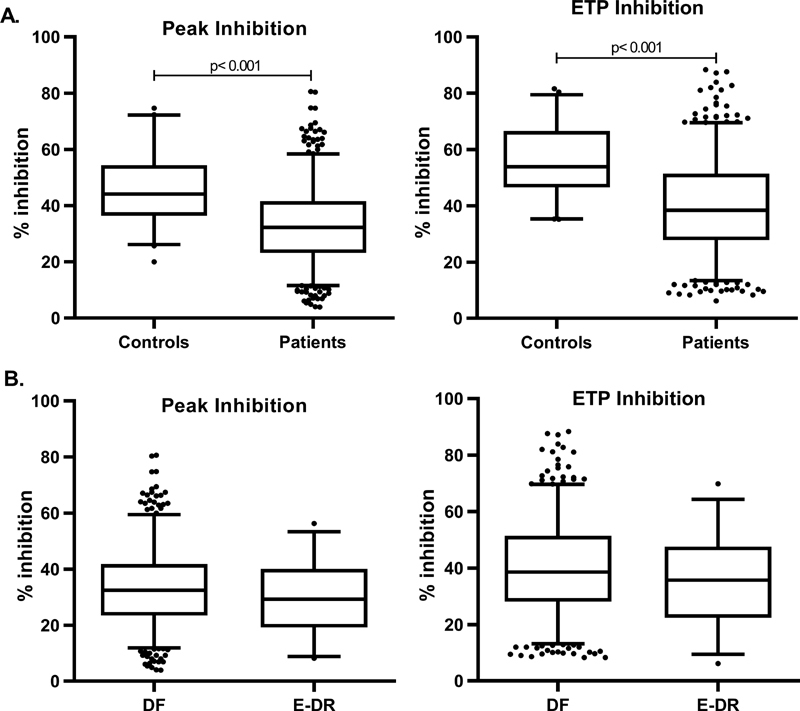
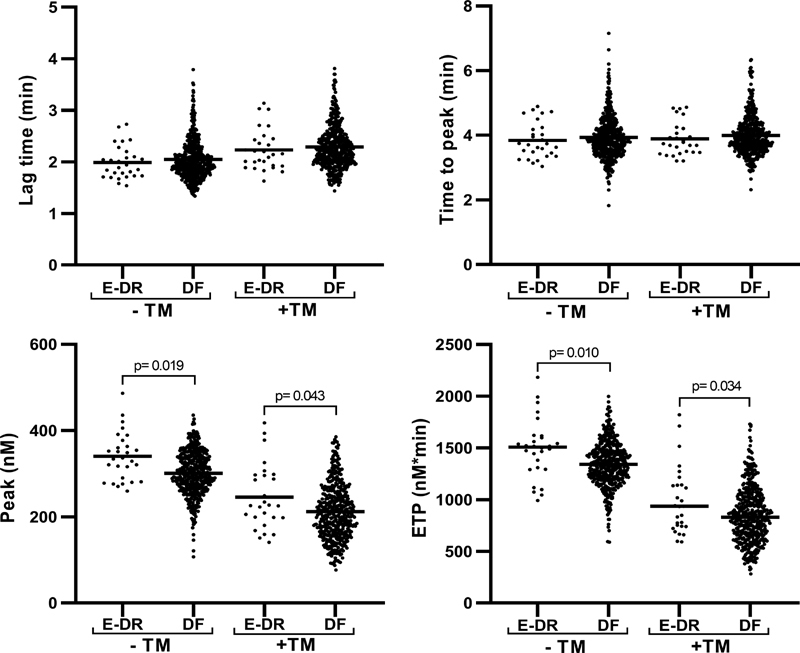
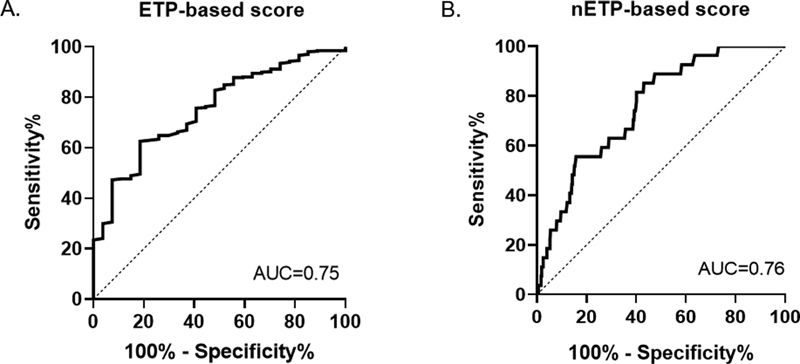
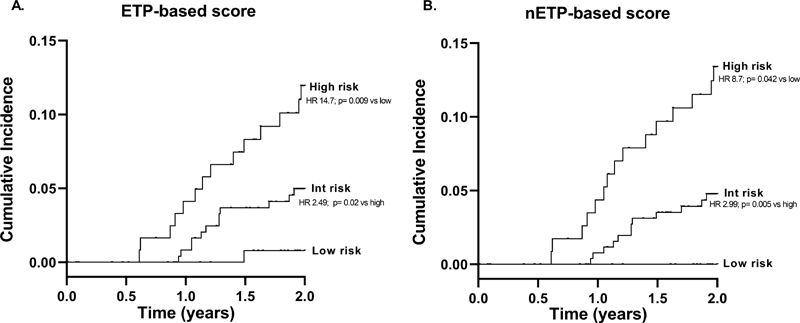
Background The measurement of thrombin generation (TG) potential by the calibrated automated thrombogram (CAT) assay provides a strong contribution in identifying patients at high risk of early disease recurrence (E-DR). However, CAT assay still needs standardization and clinical validation. Objective In this study, we aimed to validate the role of TG for E-DR prediction by means of the fully automated ST Genesia system. Methods A prospective cohort of 522 patients from the HYPERCAN study with newly diagnosed resected high-risk breast cancer was included. Fifty-two healthy women acted as controls. Plasma samples were tested for protein C, free-protein S, and TG by ST Genesia by using the STG-ThromboScreen reagent with and without thrombomodulin (TM). Results In the absence of TM, patients showed significantly higher peak and ETP compared with controls. In the presence of TM, significantly lower inhibition of ETP and Peak were observed in patients compared with controls. E-DR occurred in 28 patients; these patients had significantly higher peak and endogenous thrombin potential (ETP) in the absence of TM compared with disease-free patients. Multivariable analysis identified mastectomy, luminal B HER2-neg, triple negative subtypes, and ETP as independent risk factors for E-DR. These variables were combined to generate a risk assessment score, able to stratify patients in three-risk categories. The E-DR rates were 0, 4.7, and 13.5% in the low-, intermediate-, and high-risk categories (hazard ratio = 8.7; p < 0.05, low vs. high risk). Conclusion Our data validate the ETP parameter with a fully automated standardized system and confirm its significant contribution in identifying high-risk early breast cancer at risk for E-DR during chemotherapy.
Keywords: breast cancer; disease recurrence; hypercoagulability; risk model; thrombin generation.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. ( https://creativecommons.org/licenses/by/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures
References
-
- Eichinger S. Cancer associated thrombosis: risk factors and outcomes. Thromb Res. 2016;140 01:S12–S17. - PubMed
-
- Mahajan A, Brunson A, White R, Wun T. The epidemiology of cancer-associated venous thromboembolism: an update. Semin Thromb Hemost. 2019;45(04):321–325. - PubMed
-
- Falanga A, Russo L, Milesi V. The coagulopathy of cancer. Curr Opin Hematol. 2014;21(05):423–429. - PubMed
-
- Falanga A. Thrombophilia in cancer. Semin Thromb Hemost. 2005;31(01):104–110. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous