

Association Between Hospital Resuscitation Champion and Survival for In-Hospital Cardiac Arrest
- PMID: 33586451
- PMCID: PMC8174239
- DOI: 10.1161/JAHA.120.017509
Association Between Hospital Resuscitation Champion and Survival for In-Hospital Cardiac Arrest
Abstract
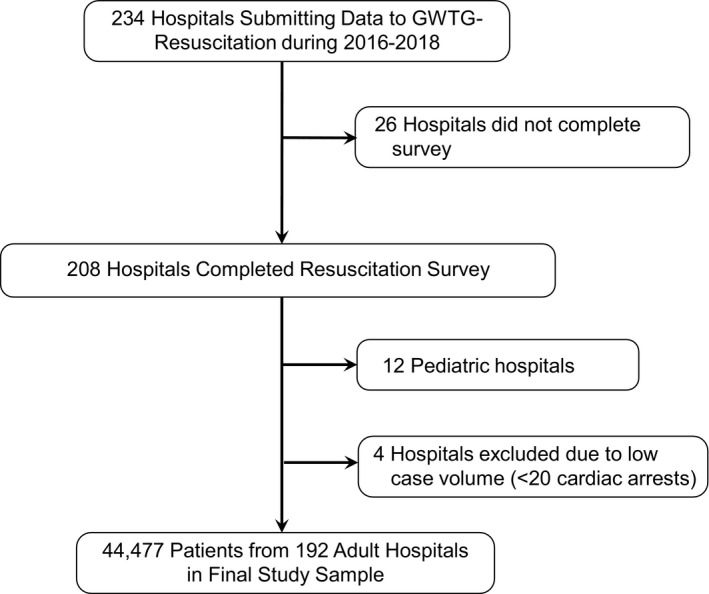
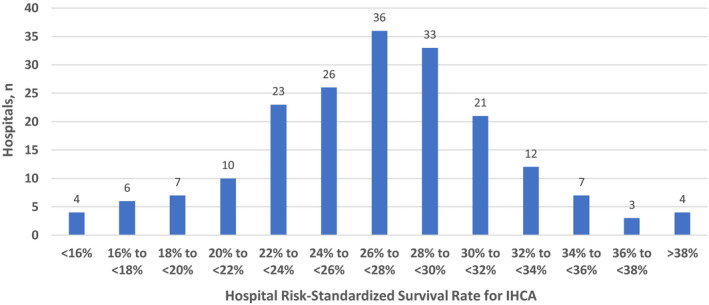
Background Although many hospitals have resuscitation champions, it is unknown if hospitals with very active physician or nonphysician champions have higher survival rates for in-hospital cardiac arrest (IHCA). Methods and Results We surveyed adult hospitals in Get With The Guidelines-Resuscitation about resuscitation practices, including about their resuscitation champion. Hospitals were categorized as having a very active physician champion, a very active nonphysician champion, or other (no champion or not very active champion). For each hospital, we calculated risk-standardized survival rates for IHCA during the period of 2016 to 2018 and categorized them into quintiles of risk-standardized survival rates. The association between a hospital's resuscitation champion type and their quintile of survival was evaluated using multivariable hierarchical proportional odds logistic regression. Overall, 192 hospitals (total of 44 477 IHCAs) comprised the study cohort. Risk-standardized survival rates for IHCA varied widely between hospitals (median: 24.7%; range: 9.2%-37.5%). Very active physician champions were present in 29 (15.1%) hospitals, 64 (33.3%) had very active nonphysician champions, and 99 (51.6%) did not have a very active champion. Compared with sites without a very active resuscitation champion, hospitals with a very active physician champion were 4 times more likely to be in a higher survival quintile, even after adjusting for resuscitation practices across hospital groups (adjusted odds ratio [OR], 3.90; 95% CI, 1.39-10.95). In contrast, there was no difference in survival between sites without very active champions and those with very active non-physician champions (adjusted OR, 1.28; 95% CI, 0.62-2.65). Conclusions The background and engagement level of a resuscitation champion is a critical factor in a hospital's survival outcomes for IHCA.
Keywords: cardiac arrest; outcomes; survival.
Conflict of interest statement
None.
Figures
Comment in
-
Building a Culture of Champions: The Importance of Leadership in Resuscitation.J Am Heart Assoc. 2021 Feb;10(5):e020390. doi: 10.1161/JAHA.121.020390. Epub 2021 Feb 15. J Am Heart Assoc. 2021. PMID: 33586452 Free PMC article. No abstract available.
References
-
- Holmberg MJ, Ross CE, Fitzmaurice GM, Chan PS, Duval‐Arnould J, Grossestreuer AV, Yankama T, Donnino MW, Andersen LW; American Heart Association's Get With The Guidelines‐Resuscitation Investigators . Annual incidence of adult and pediatric in‐hospital cardiac arrest in the United States. Circ Cardiovasc Qual Outcomes. 2019;12:e005580. - PMC - PubMed
-
- Peberdy MA, Kaye W, Ornato JP, Larkin GL, Nadkarni V, Mancini ME, Berg RA, Nichol G, Lane‐Trultt T. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58:297–308. - PubMed
-
- Cummins RO, Chamberlain D, Hazinski MF, Nadkarni V, Kloeck W, Kramer E, Becker L, Robertson C, Koster R, Zaritsky A, et al. Recommended guidelines for reviewing, reporting, and conducting research on in‐hospital resuscitation: the in‐hospital 'Utstein style'. American Heart Association. Circulation. 1997;95:2213–2239. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
