

Small Dense Low-Density Lipoprotein Cholesterol Is the Most Atherogenic Lipoprotein Parameter in the Prospective Framingham Offspring Study
- PMID: 33586462
- PMCID: PMC8174280
- DOI: 10.1161/JAHA.120.019140
Small Dense Low-Density Lipoprotein Cholesterol Is the Most Atherogenic Lipoprotein Parameter in the Prospective Framingham Offspring Study
Abstract
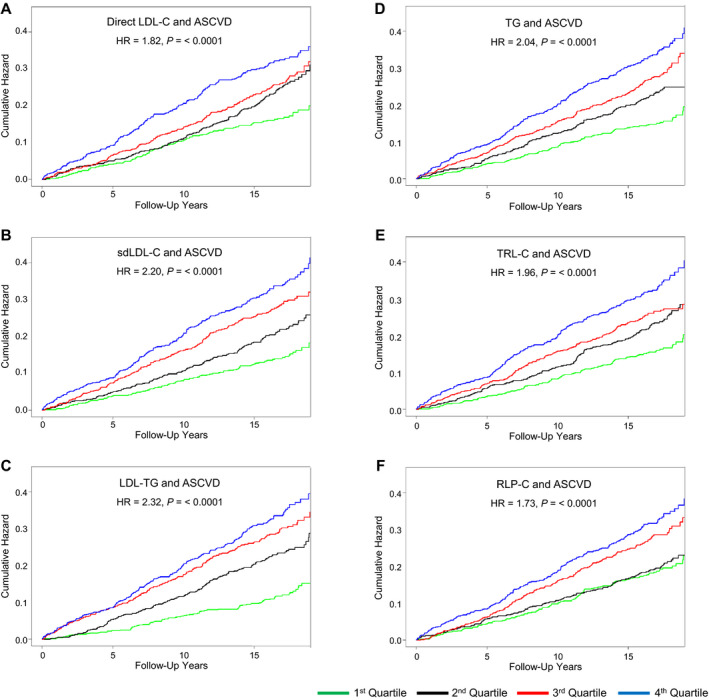
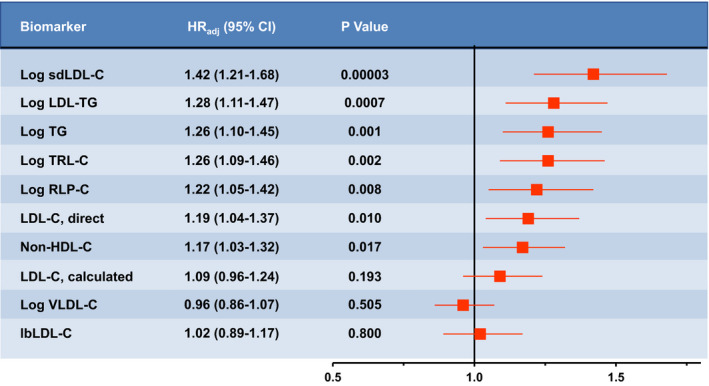
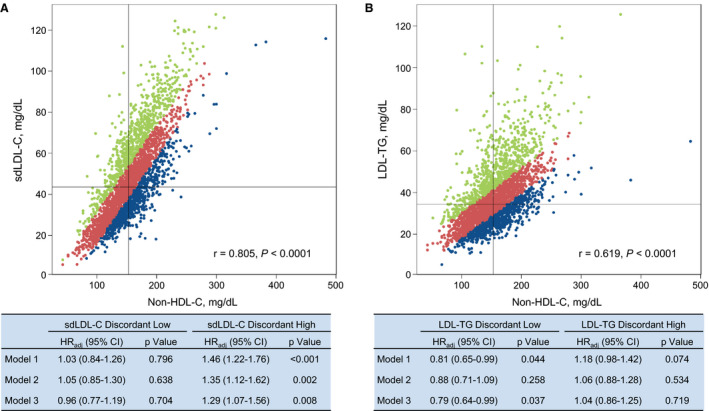
Background Elevated plasma levels of direct low-density lipoprotein cholesterol (LDL-C), small dense LDL-C (sdLDL-C), low-density lipoprotein (LDL) triglycerides, triglycerides, triglyceride-rich lipoprotein cholesterol, remnant lipoprotein particle cholesterol, and lipoprotein(a) have all been associated with incident atherosclerotic cardiovascular disease (ASCVD). Our goal was to assess which parameters were most strongly associated with ASCVD risk. Methods and Results Plasma total cholesterol, triglycerides, high-density lipoprotein cholesterol, direct LDL-C, sdLDL-C, LDL triglycerides, remnant lipoprotein particle cholesterol, triglyceride-rich lipoprotein cholesterol, and lipoprotein(a) were measured using standardized automated analysis (coefficients of variation, <5.0%) in samples from 3094 fasting subjects free of ASCVD. Of these subjects, 20.2% developed ASCVD over 16 years. On univariate analysis, all ASCVD risk factors were significantly associated with incident ASCVD, as well as the following specialized lipoprotein parameters: sdLDL-C, LDL triglycerides, triglycerides, triglyceride-rich lipoprotein cholesterol, remnant lipoprotein particle cholesterol, and direct LDL-C. Only sdLDL-C, direct LDL-C, and lipoprotein(a) were significant on multivariate analysis and net reclassification after adjustment for standard risk factors (age, sex, hypertension, diabetes mellitus, smoking, total cholesterol, and high-density lipoprotein cholesterol). Using the pooled cohort equation, many specialized lipoprotein parameters individually added significant information, but no parameter added significant information once sdLDL-C (hazard ratio, 1.42; P<0.0001) was in the model. These results for sdLDL-C were confirmed by adjusted discordance analysis versus calculated non-high-density lipoprotein cholesterol, in contrast to LDL triglycerides. Conclusions sdLDL-C, direct LDL-C, and lipoprotein(a) all contributed significantly to ASCVD risk on multivariate analysis, but no parameter added significant risk information to the pooled cohort equation once sdLDL-C was in the model. Our data indicate that small dense LDL is the most atherogenic lipoprotein parameter.
Keywords: atherosclerotic cardiovascular disease; pooled cohort equations; small dense low‐density lipoprotein cholesterol.
Conflict of interest statement
Dr Schaefer is a part‐time employee of Boston Heart Diagnostics, Framingham, MA, and has served as a consultant for the Denka Corporation, Niigata, Japan. The remaining authors have no disclosures to report.
Figures
Similar articles
-
Atherosclerotic cardiovascular disease risk and small dense low-density lipoprotein cholesterol in men, women, African Americans and non-African Americans: The pooling project.Atherosclerosis. 2023 Feb;367:15-23. doi: 10.1016/j.atherosclerosis.2023.01.015. Epub 2023 Jan 19. Atherosclerosis. 2023. PMID: 36724690
-
Small dense low-density lipoprotein as biomarker in the elderly.Clin Biochem. 2025 Jun;137:110916. doi: 10.1016/j.clinbiochem.2025.110916. Epub 2025 Mar 17. Clin Biochem. 2025. PMID: 40107376
-
Small Dense Low-Density Lipoprotein Cholesterol and Carotid Intimal Medial Thickness Progression.J Atheroscler Thromb. 2020 Oct 1;27(10):1108-1122. doi: 10.5551/jat.54130. Epub 2020 Apr 10. J Atheroscler Thromb. 2020. PMID: 32281547 Free PMC article.
-
Clinical significance of small dense low-density lipoprotein cholesterol measurement in type 2 diabetes.J Diabetes Investig. 2025 Mar;16(3):370-383. doi: 10.1111/jdi.14398. Epub 2025 Jan 7. J Diabetes Investig. 2025. PMID: 39778086 Free PMC article. Review.
-
Lowering Targeted Atherogenic Lipoprotein Cholesterol Goals for Patients at "Extreme" ASCVD Risk.Curr Diab Rep. 2019 Nov 21;19(12):146. doi: 10.1007/s11892-019-1246-y. Curr Diab Rep. 2019. PMID: 31754844 Review.
Cited by
-
Clonal hematopoiesis as a novel risk factor for type 2 diabetes mellitus in patients with hypercholesterolemia.Front Public Health. 2023 Jun 28;11:1181879. doi: 10.3389/fpubh.2023.1181879. eCollection 2023. Front Public Health. 2023. PMID: 37457265 Free PMC article.
-
Effect of PCSK9 inhibition on plasma levels of small dense low density lipoprotein-cholesterol and 7-ketocholesterol.J Clin Lipidol. 2024 Jan-Feb;18(1):e50-e58. doi: 10.1016/j.jacl.2023.10.009. Epub 2023 Oct 22. J Clin Lipidol. 2024. PMID: 37923663 Free PMC article.
-
Practical Approaches to Managing Dyslipidemia in Patients With Metabolic Dysfunction-Associated Steatotic Liver Disease.J Lipid Atheroscler. 2025 Jan;14(1):5-29. doi: 10.12997/jla.2025.14.1.5. Epub 2024 Jun 26. J Lipid Atheroscler. 2025. PMID: 39911965 Free PMC article. Review.
-
High-Density Lipoprotein Particles, Inflammation, and Coronary Heart Disease Risk.Nutrients. 2025 Mar 28;17(7):1182. doi: 10.3390/nu17071182. Nutrients. 2025. PMID: 40218941 Free PMC article.
-
Excess Triglycerides in Very Low-Density Lipoprotein (VLDL) Estimated from VLDL-Cholesterol could be a Useful Biomarker of Metabolic Dysfunction Associated Steatotic Liver Disease in Patients with Type 2 Diabetes.J Atheroscler Thromb. 2025 Feb 1;32(2):253-264. doi: 10.5551/jat.65164. Epub 2024 Sep 4. J Atheroscler Thromb. 2025. PMID: 39231648 Free PMC article.
References
-
- Goff DC Jr, Lloyd‐Jones DM, Bennett G, Coady S, D’Agostino RB, Gibbons R, Greenland P, Lackland DT, Levy D, O’Donnell CJ, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines . 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation. 2014;129:S49–S73. - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT, de Ferranti S, Faiella‐Tommasino J, Forman DE, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APHA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139:e1082–e1143. - PMC - PubMed
-
- Silverman MG, Ference BA, Im K, Wiviott SD, Giugliano RP, Grundy SM, Braunwald E, Sabatine MS. Association between lowering LDL‐C and cardiovascular risk reduction among different therapeutic interventions: a systematic review and meta‐analysis. JAMA. 2016;316:1289–1297. - PubMed
-
- Schaefer EJ, Tsunoda F, Diffenderfer MR, Polisecki EA, Thai N, Asztalos BF. The measurement of lipids, lipoproteins, apolipoproteins, fatty acids, and sterols, and next generation sequencing for the diagnosis and treatment of lipid disorders. In: Feingold KR, Anawalt B, Boyce A, Chrousos G, Dungan K, Grossman A, Hershman JM, Kaltsas G, Koch C, Kopp P, et al, eds. Endotext [Internet]. South Dartmouth, MA: MDText.com Inc; 2016:1–69. Available at: https://www.endotext.org/section/lipids. Accessed September 1, 2020.
-
- Austin MA, King MC, Vranizan KM, Krauss RM. Atherogenic lipoprotein phenotype: a proposed genetic marker for coronary heart disease risk. Circulation. 1990;82:495–506. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
