

Association of Ischemic Evaluation and Clinical Outcomes Among Patients Admitted With New-Onset Heart Failure
- PMID: 33586468
- PMCID: PMC8174286
- DOI: 10.1161/JAHA.120.019452
Association of Ischemic Evaluation and Clinical Outcomes Among Patients Admitted With New-Onset Heart Failure
Abstract
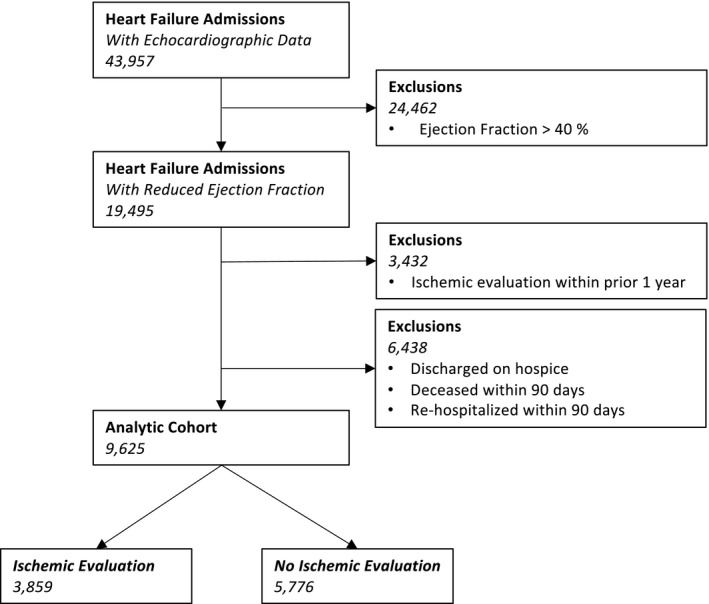
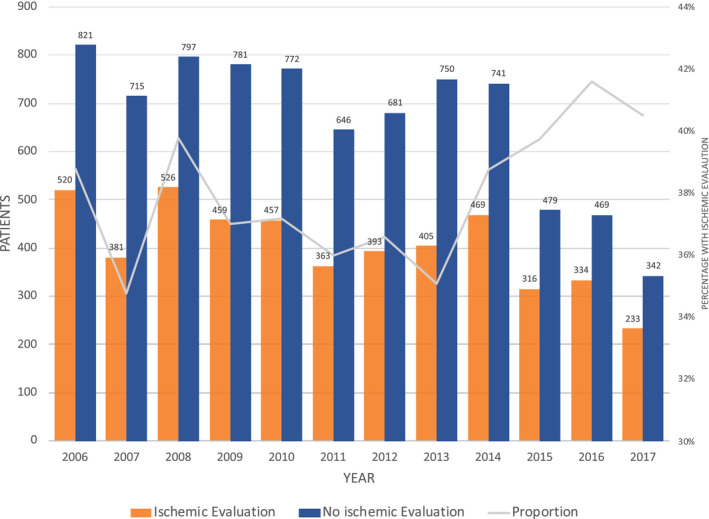
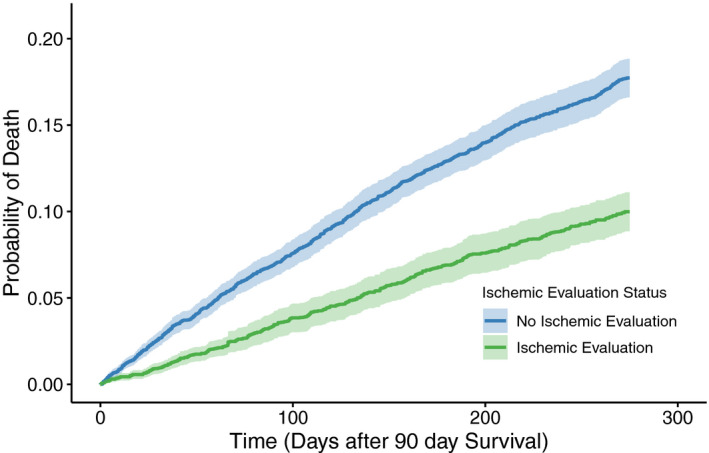
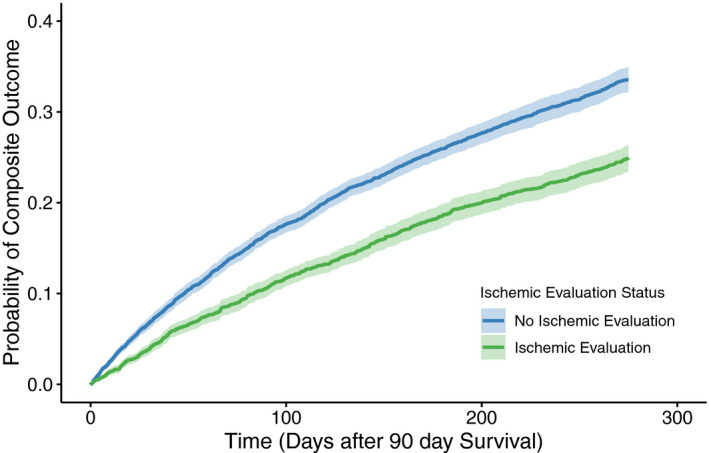
Background The significant morbidity associated with systolic heart failure makes it imperative to identify patients with a reversible cause. We thus sought to evaluate the proportion of patients who received an ischemic evaluation after a hospitalization for new-onset systolic heart failure. Methods and Results Patients admitted with a new diagnosis of heart failure and a reduction in left ventricular ejection fraction (≤40%) were identified in the VA Healthcare System from January 2006 to August 2017. Among those who survived 90 days without a readmission, we evaluated the proportion of patients who underwent an ischemic evaluation. We identified 9625 patients who were admitted with a new diagnosis of systolic heart failure with a concomitant reduction in ejection fraction. A minority of patients (3859, 40%) underwent an ischemic evaluation, with significant variation across high-performing (90th percentile) and low-performing (10th percentile) sites (odds ratio, 3.79; 95% CI, 2.90-4.31). Patients who underwent an evaluation were more likely to be treated with angiotensin-converting enzyme inhibitors (75% versus 64%, P<0.001) or beta blockers (92% versus 82%, P<0.001) and subsequently undergo percutaneous (8% versus 0%, P<0.001) or surgical (2% versus 0%, P<0.001) revascularization. Patients with an ischemic evaluation also had a significantly lower adjusted hazard of all-cause mortality (hazard ratio, 0.54; 95% CI, 0.47-0.61) compared with those without an evaluation. Conclusions Ischemic evaluations are underutilized in patients admitted with heart failure and a new reduction in left ventricular systolic function. A focused intervention to increase guideline-concordant care could lead to an improvement in clinical outcomes.
Keywords: coronary artery disease; ischemic evaluation; revascularization; systolic heart failure.
Conflict of interest statement
Dr Valle receives unrelated consulting fees from Philips Medical, Medtronic, and Cardiovascular Systems Incorporated. Dr Ho is supported by grants from NHLBI, VA HSR&D, and University of Colorado School of Medicine. He has a research agreement with Bristol‐Myers Squibb through the University of Colorado. He serves as the Deputy Editor for
Figures
References
-
- Lloyd‐Jones DM, Larson MG, Leip EP, Beiser A, D’Agostino RB, Kannel WB, Murabito JM, Vasan RS, Benjamin EJ, Levy D; Framingham Heart Study . Lifetime risk for developing congestive heart failure: the Framingham Heart Study. Circulation. 2002;106:3068–3072. DOI: 10.1161/01.CIR.0000039105.49749.6F. - DOI - PubMed
-
- Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, Chiuve SE, Cushman M, Delling FN, Deo R, et al.; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics‐2018 update: a report from the American Heart Association. Circulation. 2018;137:e67–e492. - PubMed
-
- Anderson HV, Weintraub WS, Radford MJ, Kremers MS, Roe MT, Shaw RE, Pinchotti DM, Tcheng JE. Standardized cardiovascular data for clinical research, registries, and patient care: a report from the Data Standards Workgroup of the National Cardiovascular Research Infrastructure project. J Am Coll Cardiol. 2013;61:1835–1846. DOI: 10.1016/j.jacc.2012.12.047. - DOI - PMC - PubMed
-
- Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam MA, Maddox TM, et al.; American Heart Association Advocacy Coordinating Committee, Council on Arteriosclerosis, Thrombosis and Vascular Biology, Council on Cardiovascular Radiology and Intervention, Council on Clinical Cardiology, Council on Epidemiology and Prevention, Stroke Council . Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6:606–619. DOI: 10.1161/HHF.0b013e318291329a. - DOI - PMC - PubMed
-
- Ling LF, Marwick TH, Flores DR, Jaber WA, Brunken RC, Cerqueira MD, Hachamovitch R. Identification of therapeutic benefit from revascularization in patients with left ventricular systolic dysfunction: inducible ischemia versus hibernating myocardium. Circ Cardiovasc Imaging. 2013;6:363–372. DOI: 10.1161/CIRCIMAGING.112.000138. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
