

Ferric carboxymaltose for the treatment of iron-deficient heart failure patients: a systematic review and meta-analysis
- PMID: 33586856
- PMCID: PMC7754952
- DOI: 10.1002/ehf2.13146
Ferric carboxymaltose for the treatment of iron-deficient heart failure patients: a systematic review and meta-analysis
Abstract
Aims: Intravenous ferric carboxymaltose (FCM) has been shown to improve functional capacity and quality of life in iron deficient heart failure patients. However, FCM's effect on hospitalizations and mortality remains unclear as previous randomized controlled trials (RCTs) and their meta-analyses have been underpowered to detect significant differences. We sought to conduct an updated meta-analysis using recently published RCT data.
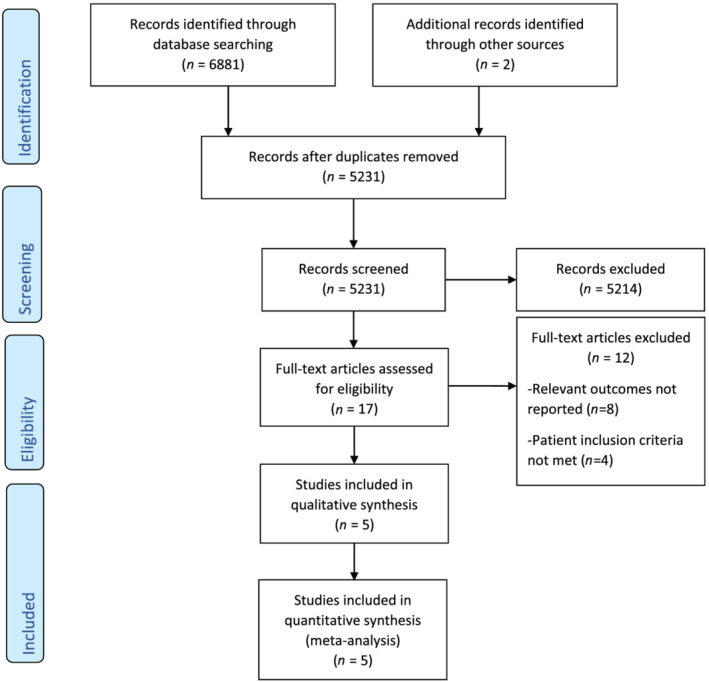
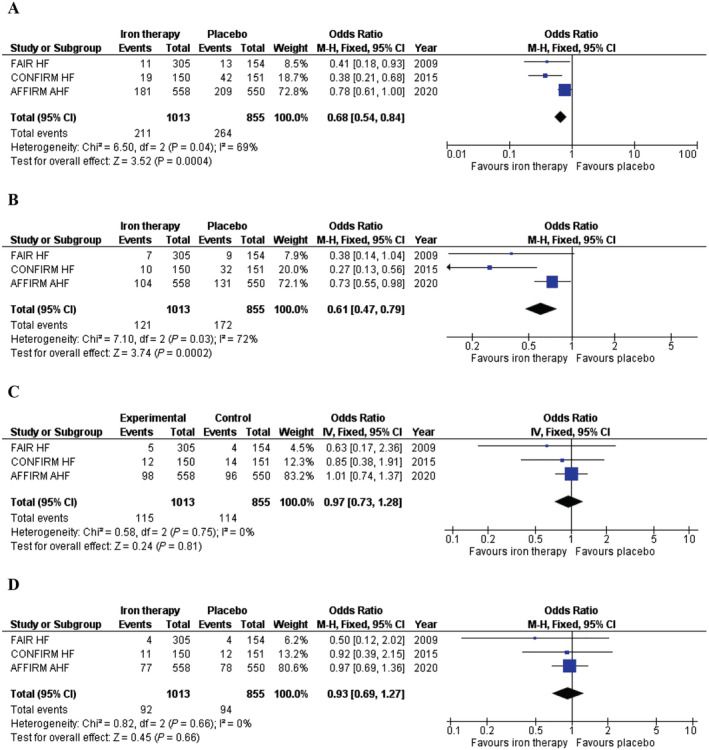
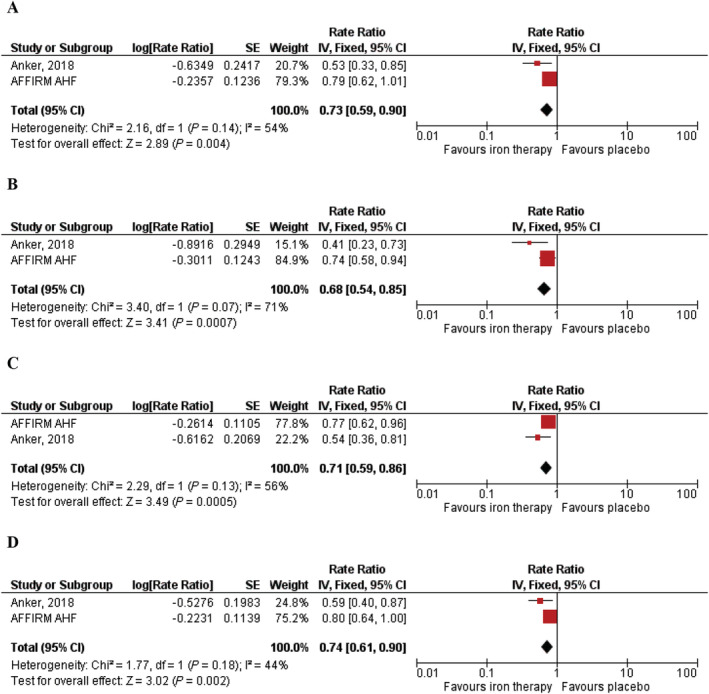
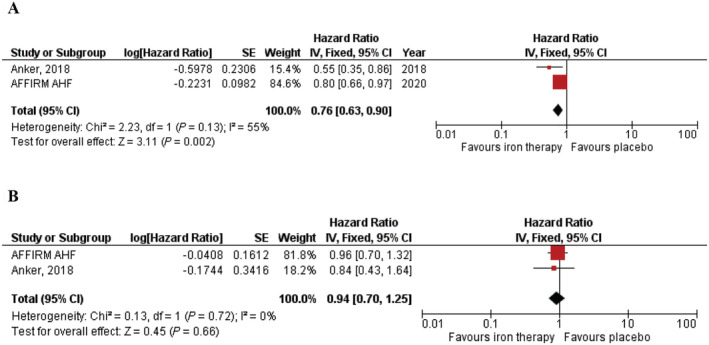
Methods and results: Online databases were searched from inception until November 2020 for RCTs evaluating the effects of FCM on clinical outcomes in iron-deficient heart failure patients. Outcomes of interest included heart failure hospitalizations, all-cause mortality, and cardiovascular mortality. Meta-analysis was performed using a fixed-effect model and estimates were reported as odds ratios (ORs), hazard ratios, or rate ratios (RRs) along with corresponding 95% confidence intervals (CIs). A total of 1947 patients (n = 1062 in the FCM group; n = 885 in the placebo group) were included. FCM, compared with placebo, significantly reduced the risk of the composite endpoint of time to first heart failure hospitalization or cardiovascular death (hazard ratio = 0.76; 95% CI = 0.63-0.90; I2 = 55%). FCM also significantly reduced the risk of recurrent heart failure hospitalizations (RR = 0.68; 95% CI = 0.54-0.85; I2 = 71%) and recurrent cardiovascular hospitalizations (RR = 0.71; 95% CI = 0.59-0.86; I2 = 56%). However, FCM had no significant effect on the risk of all-cause (OR = 0.97; 95% CI = 0.73-1.28; I2 = 0%) or cardiovascular mortality (OR = 0.93; 95% CI = 0.69-1.27; I2 = 0%).
Conclusions: Ferric carboxymaltose reduces heart failure hospitalizations and cardiovascular hospitalizations with no beneficial effect on all-cause and cardiovascular mortality in iron-deficient heart failure patients. These findings reinforce the role of FCM as a therapeutic option in heart failure patients.
Keywords: Heart failure; Iron deficiency; Iron therapy; Meta‐analysis.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
WD reports speaker fees and advisory honoraria from Aimediq, Bayer, Boehringer Ingelheim, Lilly, Medtronic, Pfizer, Sanofi‐Aventis, Sphingotec, Vifor Pharma. WD reports research support from EU (Horizon2020), German ministry of Education and Research, German Center for Cardiovascular Research, Vifor Pharma, ZS Pharma.
Figures
References
-
- Anand IS, Gupta P. Anemia and iron deficiency in heart failure: current concepts and emerging therapies. Circulation 2018; 138: 80–98. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016; 37: 2129–2200. - PubMed
-
- Anker SD, Comin Colet J, Filippatos G, Willenheimer R, Dickstein K, Drexler H, Lüscher TF, Bart B, Banasiak W, Niegowska J, Kirwan BA, Mori C, von Eisenhart Rothe B, Pocock SJ, Poole‐Wilson PA, Ponikowski P. Ferric carboxymaltose in patients with heart failure and iron deficiency. N Engl J Med 2009; 361: 2436–2448. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
