

Efficacy and safety of SGLT2 inhibitors in heart failure: systematic review and meta-analysis
- PMID: 33586910
- PMCID: PMC7755023
- DOI: 10.1002/ehf2.13169
Efficacy and safety of SGLT2 inhibitors in heart failure: systematic review and meta-analysis
Erratum in
-
Corrigendum.ESC Heart Fail. 2021 Jun;8(3):2362. doi: 10.1002/ehf2.13338. Epub 2021 May 1. ESC Heart Fail. 2021. PMID: 33931956 Free PMC article. No abstract available.
Abstract
Aims: We sought to conduct a meta-analysis regarding the safety and efficacy of sodium-glucose co-transporter 2 (SGLT2) inhibitors in patients with heart failure (HF).
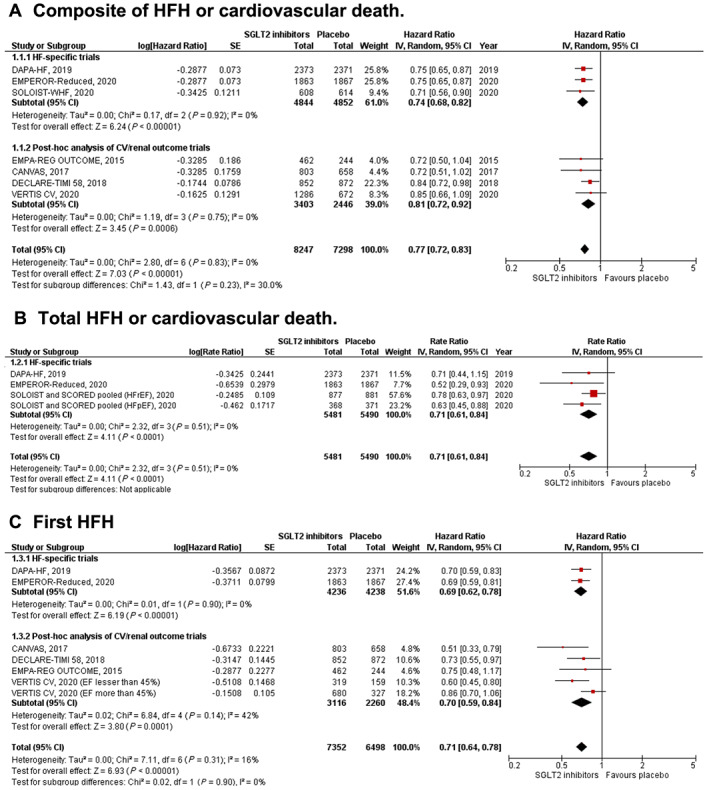
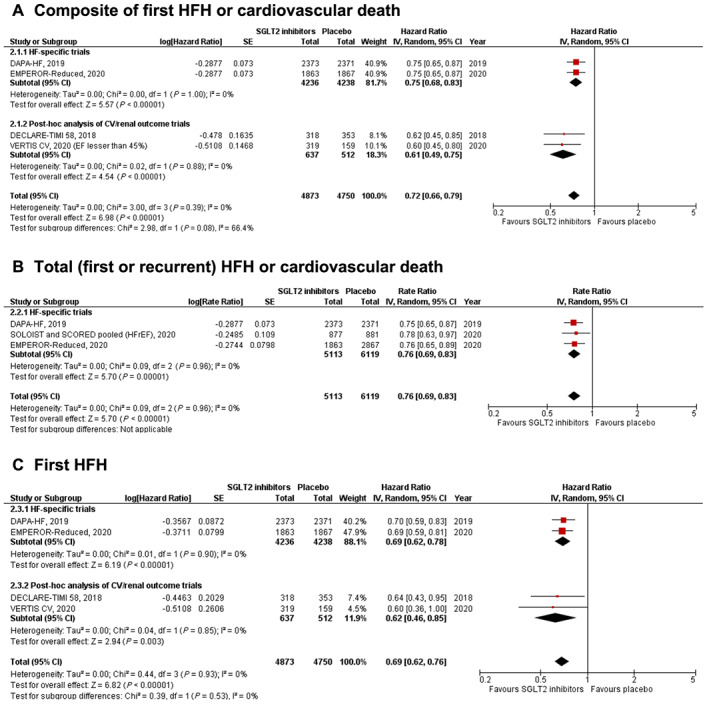
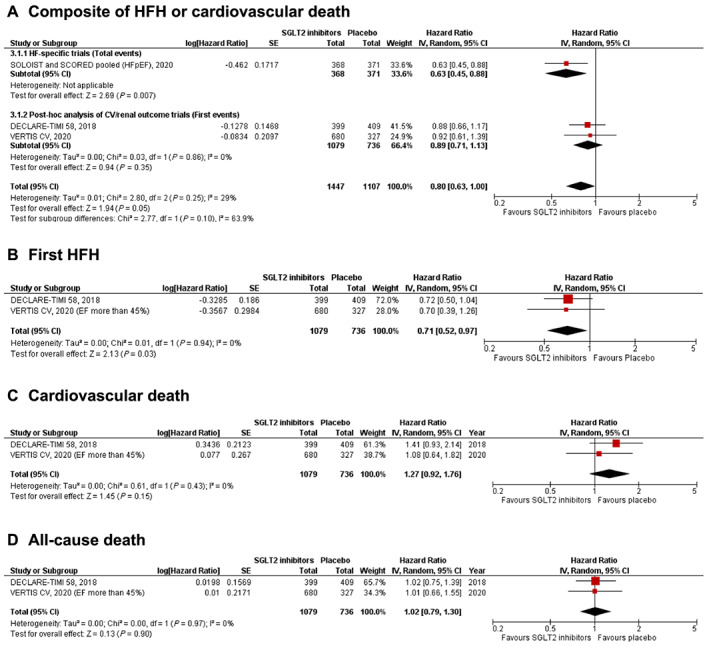
Methods and results: MEDLINE, Scopus, Cochrane CENTRAL, and ClinicalTrials.gov were searched from their inception to November 2020 for placebo-controlled randomized controlled trials of SGLT2 inhibitors. Randomized controlled trials were selected if they reported at least one of the prespecified outcomes in patients with HF. Hazard ratios (HRs) or risk ratios and their corresponding 95% confidence intervals were pooled using a random-effects model. A total of seven trials including 16 820 HF patients (N = 8884 in the SGLT2 inhibitor arms; N = 7936 in the placebo arms) were included. In the overall HF cohort, SGLT2 inhibitors compared with placebo significantly reduced the risk of the composite endpoint of first HF hospitalization or cardiovascular death [HR: 0.77 (0.72-0.83); P < 0.001; I2 = 0%], time to first HF hospitalization [HR: 0.71 (0.64-0.78); P < 0.001; I2 = 0], cardiovascular mortality [HR: 0.87 (0.79-0.96); P = 0.005; I2 = 0%], and all-cause mortality [HR: 0.89 (0.82-0.96); P = 0.004; I2 = 0%]. Results remained consistent across HF-specific trials and according to diabetes mellitus status. A trend towards benefit was observed in patients with HF with preserved ejection fraction for the composite of HF hospitalization and cardiovascular death [HR: 0.80 (0.63-1.00); P = 0.05; I2 = 29%]. No increased risk of hypovolaemia, hyperkalaemia, and hypotension was seen with SGLT2 inhibitors compared with placebo.
Conclusions: SGLT2 inhibitors significantly improve cardiovascular outcomes including cardiovascular and all-cause mortality in patients with HF without an increased risk of serious adverse events. A trend towards benefit was observed in patients with HF with preserved ejection fraction.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
J.B. is a consultant for Abbott, Amgen, Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squib, CVRx, Janssen, LivaNova, Luitpold, Medtronic, Merck, Novartis, Relypsa, and Vifor. S.J.G. was supported by Heart Failure Society of America/Emergency Medicine Foundation Acute Heart Failure Young Investigator Award funded by Novartis, has received research support from Amgen, Bristol‐Myers Squibb, and Novartis, and serves on an advisory board for Amgen. M.V. is supported by the KL2/Catalyst Medical Research Investigator Training award from Harvard Catalyst (NIH/NCATS Award UL 1TR002541), serves on advisory boards for Amgen, AstraZeneca, Baxter Healthcare, Bayer AG, Boehringer Ingelheim, Cytokinetics, and Relypsa, and participates on clinical endpoint committees for studies sponsored by Galmed, Novartis, and the NIH. T.F. reports personal fees from Novartis, Bayer, Janssen, SGS, Roche, Boehringer Ingelheim, Daiichi‐Sankyo, Galapagos, Penumbra, Parexel, Vifor, BiosenseWebster, CSL Behring, Fresenius Kabi, Coherex Medical, and LivaNova. G.F. participated in committees of trials and registries sponsored by BI, Bayer, Medtronic, Servier, Novartis, and Vifor. A.J.S.C. reports honoraria and/or lecture fees from AstraZeneca, Bayer, Menarini, Novartis, Nutricia, Servier, Vifor, Actimed, Cardiac Dimensions, CVRx, Enopace, Faraday, Gore, Impulse Dynamics, Respicardia, Stealth Peptides, V‐Wave, Corvia, Arena, and ESN Cleer. S.D.A. has received research support from Vifor International & Abbott Vascular and fees for consultancy and/or speaking from Astra‐Zeneca, Bayer, Boehringer Ingelheim, Respicardia, Impulse Dynamics, Janssen, Novartis, Servier, and Vifor International. All other authors report no disclosures.
Figures
References
-
- Usman MS, Siddiqi TJ, Memon MM, Khan MS, Rawasia WF, Talha Ayub M, Sreenivasan J, Golzar Y. Sodium‐glucose co‐transporter 2 inhibitors and cardiovascular outcomes: a systematic review and meta‐analysis. Eur J Prev Cardiol 2018; 25: 495–502. - PubMed
-
- Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, Shaw W, Law G, Desai M, Matthews DR. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017; 377: 644–657. - PubMed
-
- Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, Broedl UC, Inzucchi SE. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015; 373: 2117–2128. - PubMed
-
- Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Silverman MG, Zelniker TA, Kuder JF, Murphy SA, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Ruff CT, Gause‐Nilsson IAM, Fredriksson M, Johansson PA, Langkilde AM, Sabatine MS. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019; 380: 347–357. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
