

Imaging foreign bodies in head and neck trauma: a pictorial review
- PMID: 33587198
- PMCID: PMC7884531
- DOI: 10.1186/s13244-021-00969-9
Imaging foreign bodies in head and neck trauma: a pictorial review
Abstract
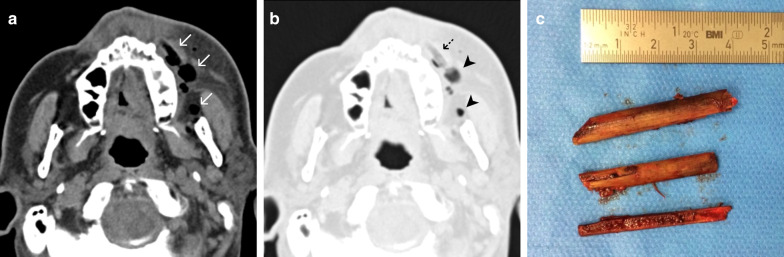
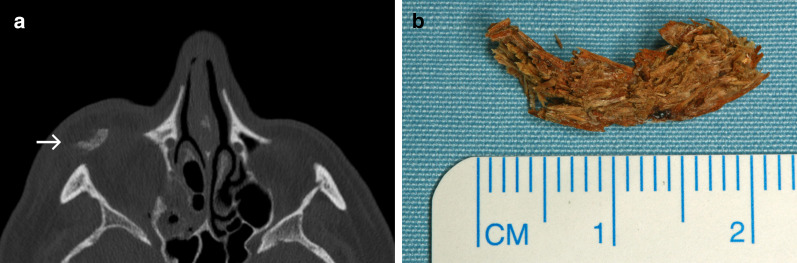
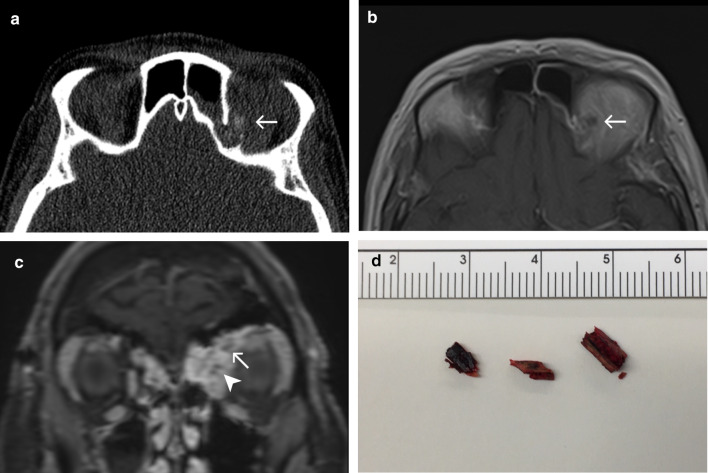
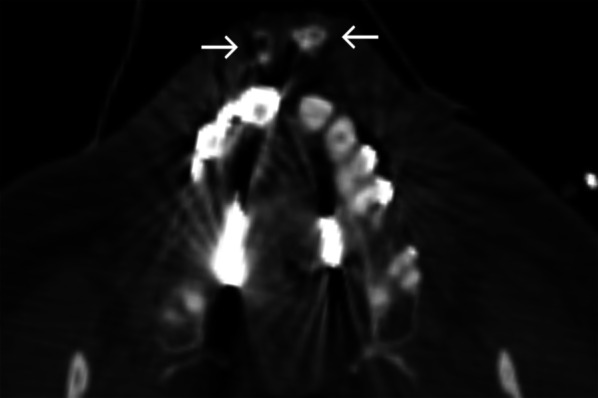
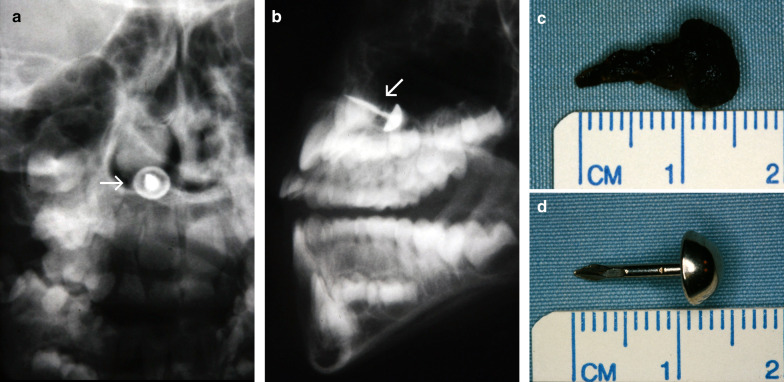
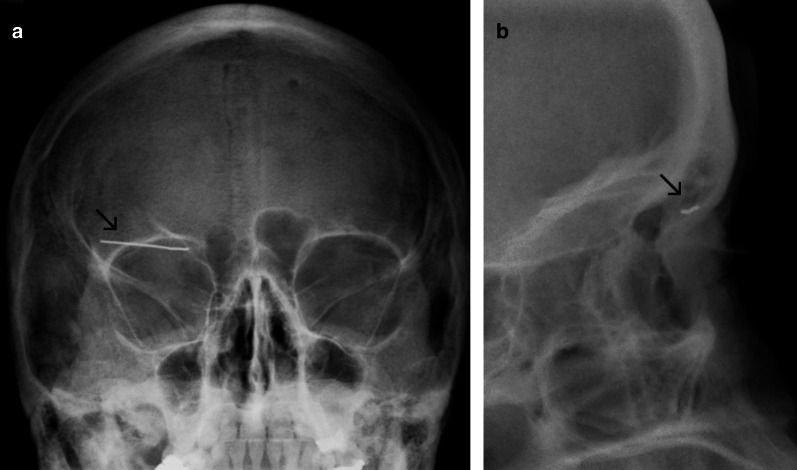
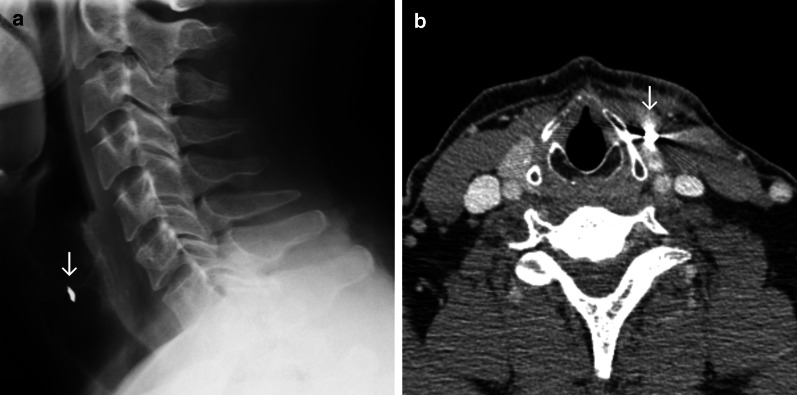
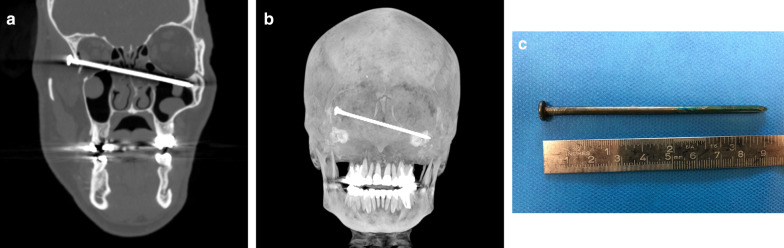
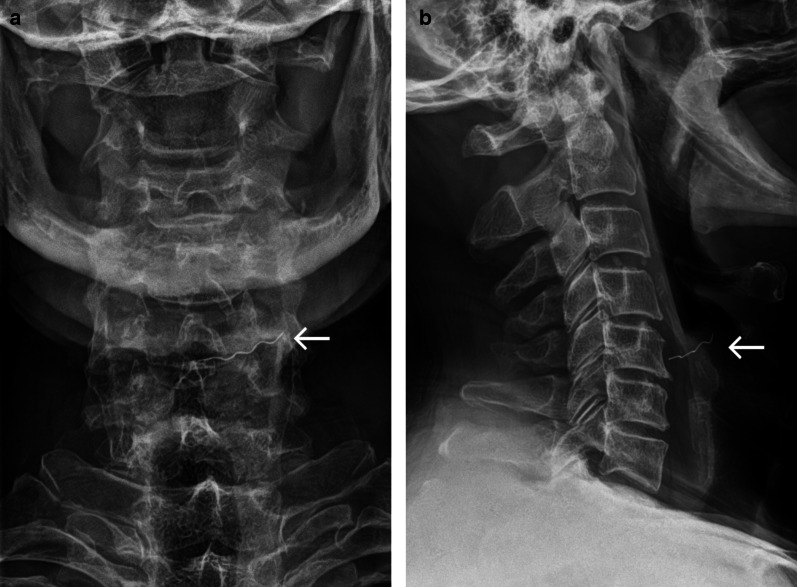
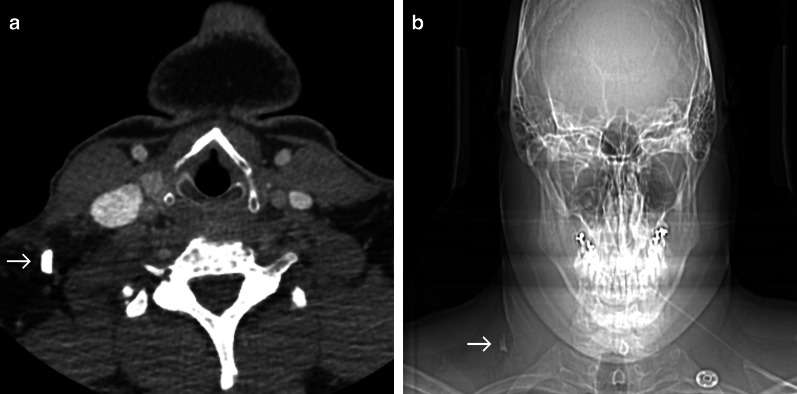
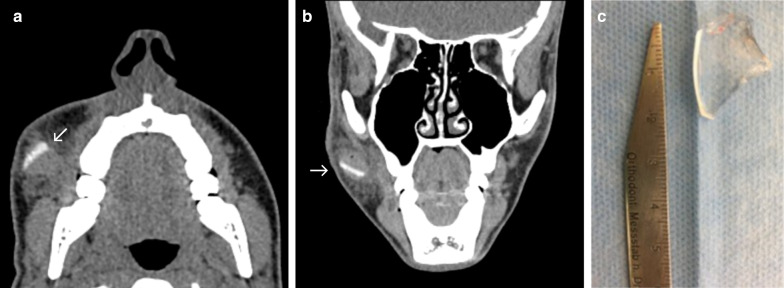
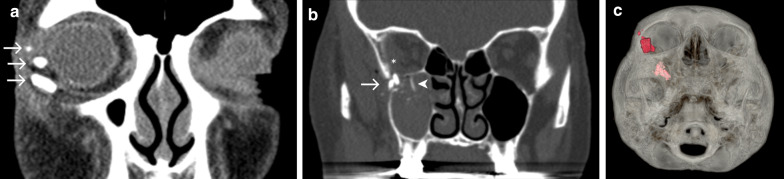
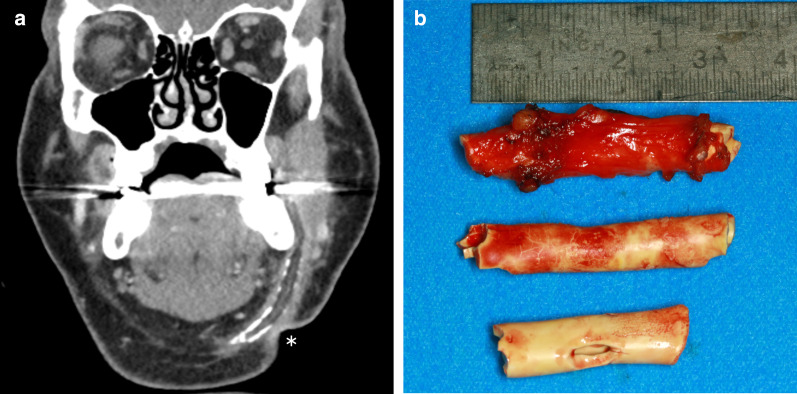
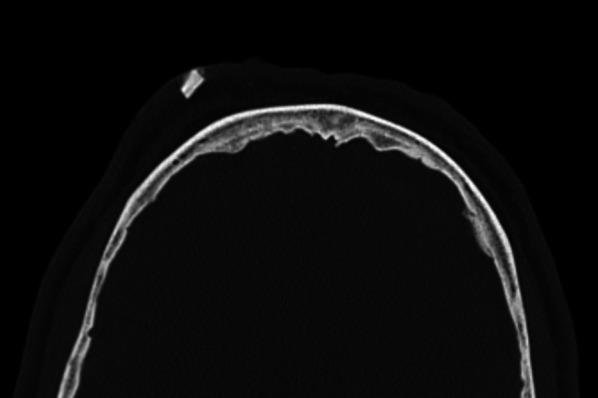
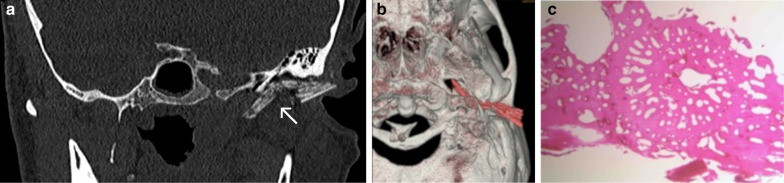
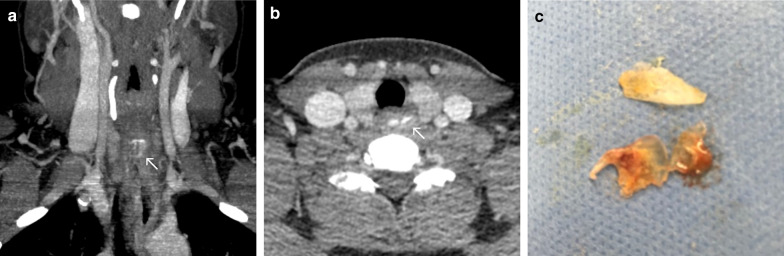
Open injuries bear the risk of foreign body contamination. Commonly encountered materials include gravel debris, glass fragments, wooden splinters or metal particles. While foreign body incorporation is obvious in some injury patterns, other injuries may not display hints of being contaminated with foreign body materials. Foreign objects that have not been detected and removed bear the risk of leading to severe wound infections and chronic wound healing disorders. Besides these severe health issues, medicolegal consequences should be considered. While an accurate clinical examination is the first step for the detection of foreign body materials, choosing the appropriate radiological imaging is decisive for the detection or non-detection of the foreign material. Especially in cases of impaired wound healing over time, the existence of an undetected foreign object needs to be considered.Here, we would like to give a practical radiological guide for the assessment of foreign objects in head and neck injuries by a special selection of patients with different injury patterns and various foreign body materials with regard to the present literature.
Keywords: Dislocated foreign body; Foreign body injuries; Imaging foreign bodies; Penetrating injury.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Bartholomew BJ, Poole C, Tayag EC (2003) Unusual transoral penetrating injury of the foramen magnum: case report. Neurosurgery 53:989–991 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
