

Primary breast tuberculosis: imaging findings of a rare disease
- PMID: 33587199
- PMCID: PMC7884561
- DOI: 10.1186/s13244-021-00961-3
Primary breast tuberculosis: imaging findings of a rare disease
Abstract
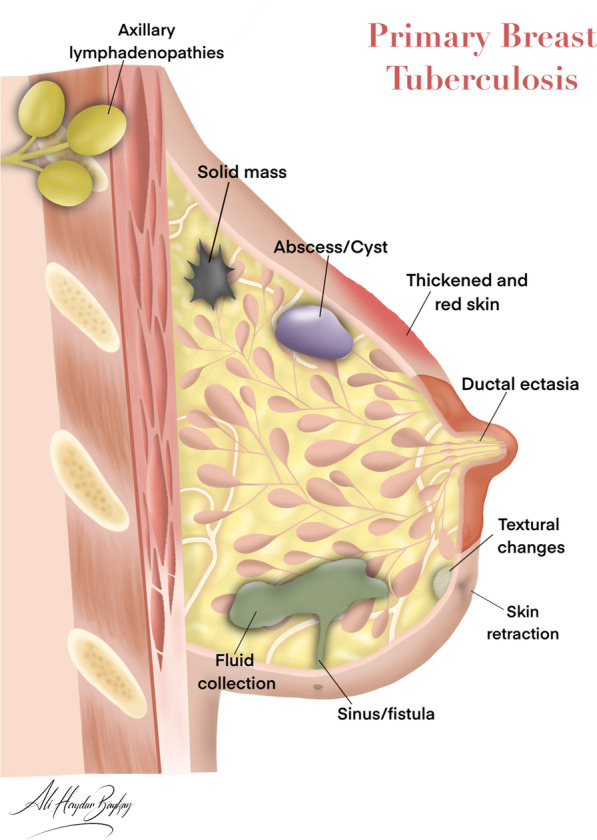
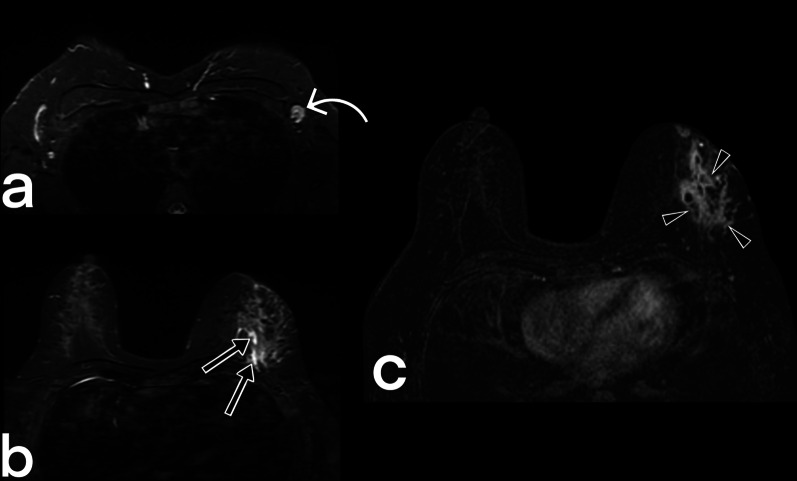
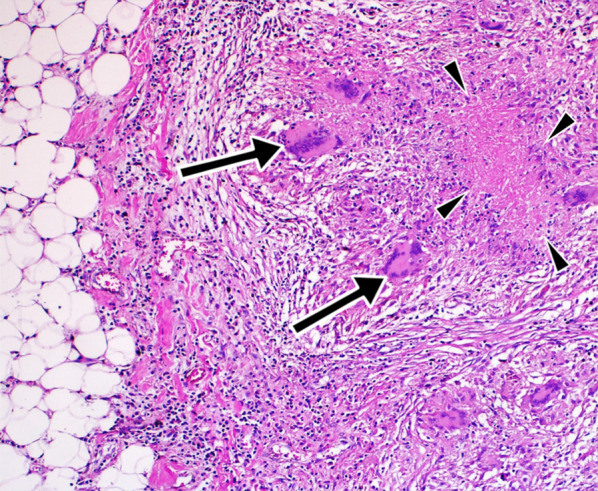
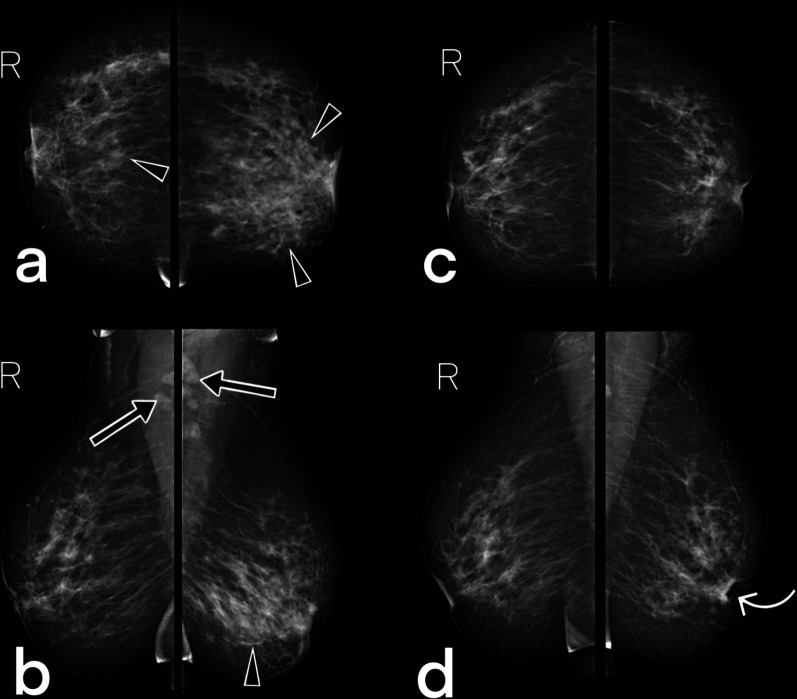
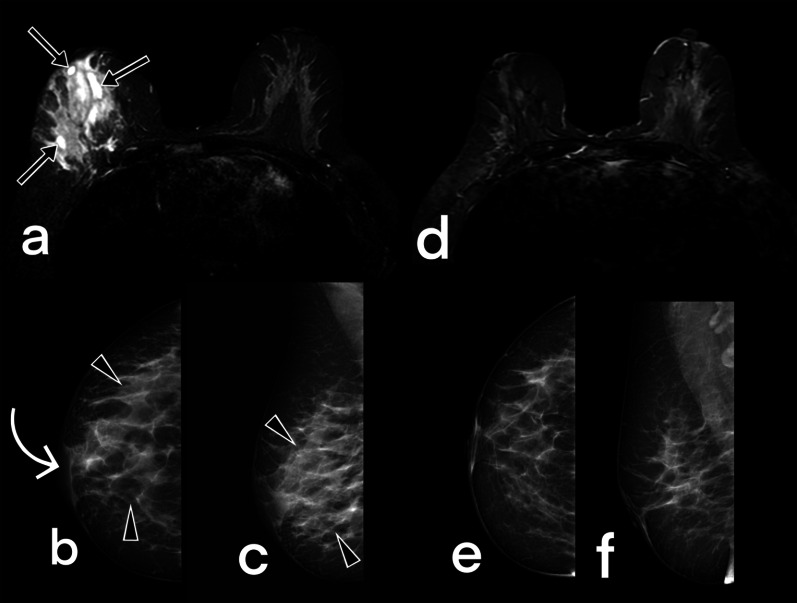
Breast tuberculosis is a rare form of extrapulmonary tuberculosis which tends to affect females of reproductive age, and is much rarer in males, postmenopausal women, and pre-pubescent girls. It is difficult to diagnose because it can mimic benign conditions such as a fibroadenoma, as well as malignant diseases like a carcinoma. It is also particularly difficult to distinguish breast tuberculosis from granulomatous mastitis, so other possible diagnoses should be ruled out first. The diagnosis of breast tuberculosis has three essential pillars: clinical examination, radiological evaluations, and histopathological sampling. Radiological evaluations are not only critical in diagnosis but are also important in the planning of the treatment and during the follow-up. This paper aims to review the imaging findings and the differential diagnosis of breast tuberculosis.
Keywords: Breast; Extrapulmonary tuberculosis; Mammography; Tuberculosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures








References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
